

Optimal dosage and route of administration of methotrexate in rheumatoid arthritis: a systematic review of the literature
- PMID: 19033290
- PMCID: PMC2689521
- DOI: 10.1136/ard.2008.092668
Optimal dosage and route of administration of methotrexate in rheumatoid arthritis: a systematic review of the literature
Abstract
Objectives: To review systematically the available literature on the optimal dosage and route of administration of methotrexate in patients with rheumatoid arthritis (RA), as an evidence base for generating clinical practice recommendations.
Methods: A systematic literature search was carried out in MEDLINE, EMBASE, Cochrane Library and American College of Rheumatology/European League Against Rheumatism meeting abstracts, searching for randomised controlled trials evaluating various dosages or routes of administration of methotrexate in RA. Articles that fulfilled predefined inclusion criteria were systematically reviewed and the quality was appraised. Effect sizes and odds ratios for clinical, radiological and toxicity outcomes were calculated and directly or indirectly compared between study groups using methotrexate in different dosages or by different routes.
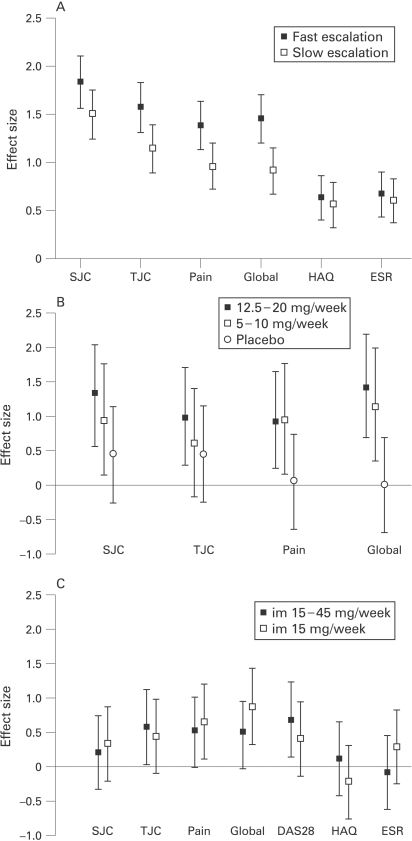
Results: A total of 38 publications out of 1748 identified references was included in the review. Start doses of 25 mg/week or fast escalation with 5 mg/month to 25-30 mg/week were associated with higher clinical effect sizes and more (gastrointestinal) adverse events in comparison with doses of 5-15 mg/week or slow escalation. Starting with 15 mg/week subcutaneous versus oral methotrexate was associated with higher clinical efficacy but more withdrawal due to toxicity in early RA. In longstanding RA, after failure on 15-20 mg/week orally, a switch to 15 mg/week intramuscularly with subsequent dose escalation did not result in increased efficacy.
Conclusions: Starting on methotrexate 15 mg/week orally, escalating with 5 mg/month to 25-30 mg/week, or the highest tolerable dose, with a subsequent switch to subcutaneous administration in the case of an insufficient response, seems to be the optimal evidence-based dosing and routing recommendation for methotrexate in RA.
Conflict of interest statement
Figures
References
-
- Aletaha D, Smolen JS. The rheumatoid arthritis patient in the clinic: comparing more than 1,300 consecutive DMARD courses. Rheumatology (Oxford) 2002;41:1367–74 - PubMed
-
- Maetzel A, Wong A, Strand V, Tugwell P, Wells G, Bombardier C. Meta-analysis of treatment termination rates among rheumatoid arthritis patients receiving disease-modifying anti-rheumatic drugs. Rheumatology (Oxford) 2000;39:975–81 - PubMed
-
- Weinblatt ME. Efficacy of methotrexate in rheumatoid arthritis. Br J Rheumatol 1995;34(suppl 2):43–8 - PubMed
-
- Visser K, Katchamart W, Loza E, Martinez-Lopez JA, Salliot C, Trudeau J, et al. Multinational evidence-based recommendations for the use of methotrexate in rheumatic disorders with a focus on rheumatoid arthritis: integrating systematic literature research and expert opinion of a broad international panel of rheumatologists in the 3E Initiative. Ann Rheum Dis 2009;68:1086–93 - PMC - PubMed
-
- van Tulder M, Furlan A, Bombardier C, Bouter L. Updated method guidelines for systematic reviews in the Cochrane Collaboration Back Review Group. Spine 2003;28:1290–9 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
