

Disparities in liver transplantation before and after introduction of the MELD score
- PMID: 19033587
- PMCID: PMC3640479
- DOI: 10.1001/jama.2008.720
Disparities in liver transplantation before and after introduction of the MELD score
Abstract
Context: In February 2002, the allocation system for liver transplantation became based on the Model for End-Stage Liver Disease (MELD) score. Before MELD, black patients were more likely to die or become too sick to undergo liver transplantation compared with white patients. Little information exists regarding sex and access to liver transplantation.
Objective: To determine the association between race, sex, and liver transplantation following introduction of the MELD system.
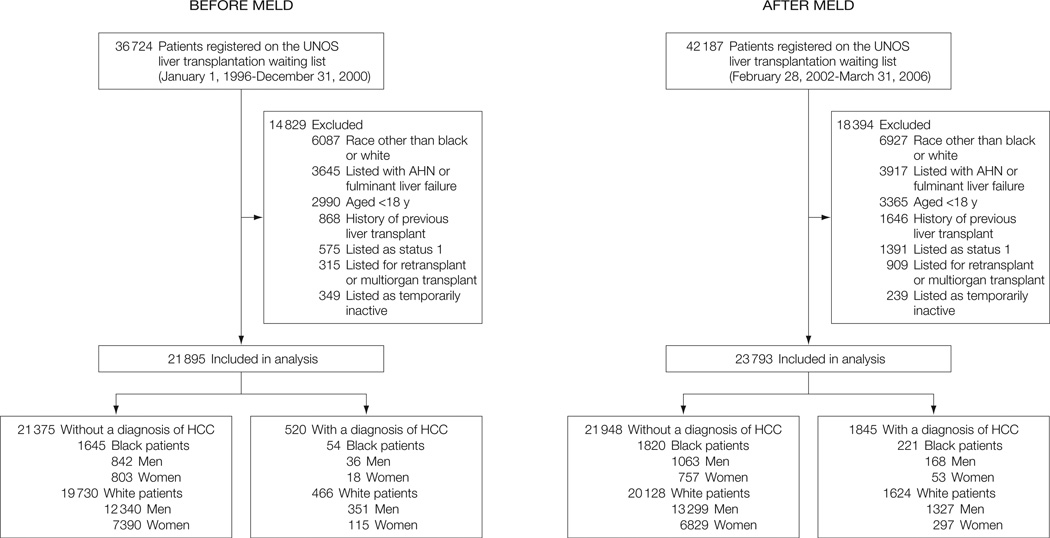
Design, setting, and patients: A retrospective cohort of black and white patients (> or = 18 years) registered on the United Network for Organ Sharing liver transplantation waiting list between January 1, 1996, and December 31, 2000 (pre-MELD cohort, n = 21 895) and between February 28, 2002, and March 31, 2006 (post-MELD cohort, n = 23 793).
Main outcome measures: Association between race, sex, and receipt of a liver transplant. Separate multivariable analyses evaluated cohorts within each period to identify predictors of time to death and the odds of dying or receiving liver transplantation within 3 years of listing. Patients with hepatocellular carcinoma were analyzed separately.
Results: Black patients were younger (mean [SD], 49.2 [10.7] vs 52.4 [9.2] years; P < .001) and sicker (MELD score at listing: median [interquartile range], 16 [12-22] vs 14 [11-19]; P < .001) than white patients on the waiting list for both periods. In the pre-MELD cohort, black patients were more likely to die or become too sick for liver transplantation than white patients (27.0% vs 21.7%) within 3 years of registering on the waiting list (odds ratio [OR], 1.51; 95% confidence interval (CI), 1.15-1.98; P = .003). In the post-MELD cohort, black race was no longer associated with increased likelihood of death or becoming too sick for liver transplantation (26.5% vs 22.0%, respectively; OR, 0.96; 95% CI, 0.74-1.26; P = .76). Black patients were also less likely to receive a liver transplant than white patients within 3 years of registering on the waiting list pre-MELD (61.6% vs 66.9%; OR, 0.75; 95% CI, 0.59-0.97; P = .03), whereas post-MELD, race was no longer significantly associated with receipt of a liver transplant (47.5% vs 45.5%, respectively; OR, 1.04; 95% CI, 0.84-1.28; P = .75). Women were more likely than men to die or become too sick for liver transplantation post-MELD (23.7% vs 21.4%; OR, 1.30; 95% CI, 1.08-1.47; P = .003) vs pre-MELD (22.4% vs 21.9%; OR, 1.08; 95% CI, 0.91-1.26; P = .37). Similarly, women were less likely than men to receive a liver transplant within 3 years both pre-MELD (64.8% vs 67.6%; OR, 0.80; 95% CI, 0.70-0.92; P = .002) and post-MELD (39.9% vs 48.7%; OR, 0.70; 95% CI, 0.62-0.79; P < .001).
Conclusion: Following introduction of the MELD score to the liver transplantation allocation system, race was no longer associated with receipt of a liver transplant or death on the waiting list, but disparities based on sex remain.
Figures
Comment in
-
Race and sex disparities in liver transplantation: progress toward achieving equal access?JAMA. 2008 Nov 26;300(20):2425-6. doi: 10.1001/jama.2008.732. JAMA. 2008. PMID: 19033595 No abstract available.
-
Disparities in liver transplantation in the post-model for end-stage liver disease era: are we there yet?Hepatology. 2009 Sep;50(3):981-4. doi: 10.1002/hep.22939. Hepatology. 2009. PMID: 19670420 No abstract available.
References
-
- Malinchoc M, Kamath PS, Gordon FD, Peine CJ, Rank J, terBorg PL. A model to predict poor survival in patients undergoing transjugular intrahepatic portosystemic shunts. Hepatology. 2000;31(4):864–871. - PubMed
-
- Wiesner R, Edwards E, Freeman R, et al. Model for end stage liver disease (MELD) and allocation of donor livers. Gastroenterology. 2003;124(1):91–96. - PubMed
-
- Institute of Medicine Committee on Organ Procurement and Transplantation Policy. Organ Procurement and Transplantation: Assessing Current Policies and the Potential Impact of the DHHS Final Rule. Washington, DC: National Academy Press; 1999. pp. 1–29. - PubMed
-
- Freeman RB, Wiesner RH, Edwards E, Harper A, Merion R, Wolfe R. Results of the first year of the new liver allocation plan. Liver Transpl. 2004;10(1):7–15. - PubMed
-
- Kanwal F, Dulai GS, Spiegel BMR, Yee HF, Gralnek IM. A comparison of liver transplantation outcomes in the pre- vs. post-MELD eras. Aliment Pharmacol Ther. 2005;21(2):169–177. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
