

Inhaled corticosteroids in patients with stable chronic obstructive pulmonary disease: a systematic review and meta-analysis
- PMID: 19033591
- PMCID: PMC4804462
- DOI: 10.1001/jama.2008.717
Inhaled corticosteroids in patients with stable chronic obstructive pulmonary disease: a systematic review and meta-analysis
Erratum in
- JAMA. 2009 Mar 11;301(10):1024
Abstract
Context: Recent studies of inhaled corticosteroid (ICS) therapy for managing stable chronic obstructive pulmonary disease (COPD) have yielded conflicting results regarding survival and risk of adverse events.
Objective: To systematically review and quantitatively synthesize the effects of ICS therapy on mortality and adverse events in patients with stable COPD.
Data sources: Search of MEDLINE, CENTRAL, EMBASE, CINAHL, Web of Science, and PsychInfo through February 9, 2008.
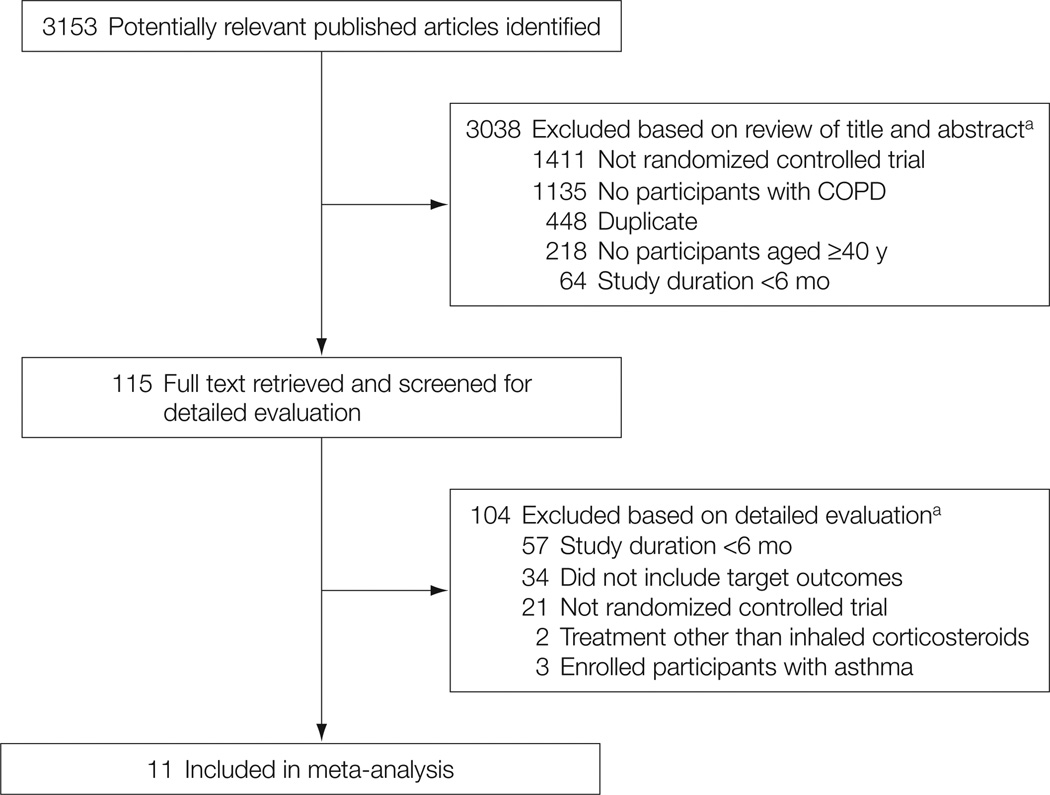
Study selection: Eligible studies were double-blind, randomized controlled trials comparing ICS therapy for 6 or more months with nonsteroid inhaled therapy in patients with COPD.
Data extraction: Two authors independently abstracted data including study characteristics, all-cause mortality, pneumonia, and bone fractures. The I(2) statistic was used to assess heterogeneity. Study-level data were pooled using a random-effects model (when I(2) > or = 50%) or a fixed-effects model (when I(2) < 50%). For the primary outcome of all-cause mortality at 1 year, our meta-analysis was powered to detect a 1.0% absolute difference in mortality, assuming a 2-sided alpha of .05 and power of 0.80.
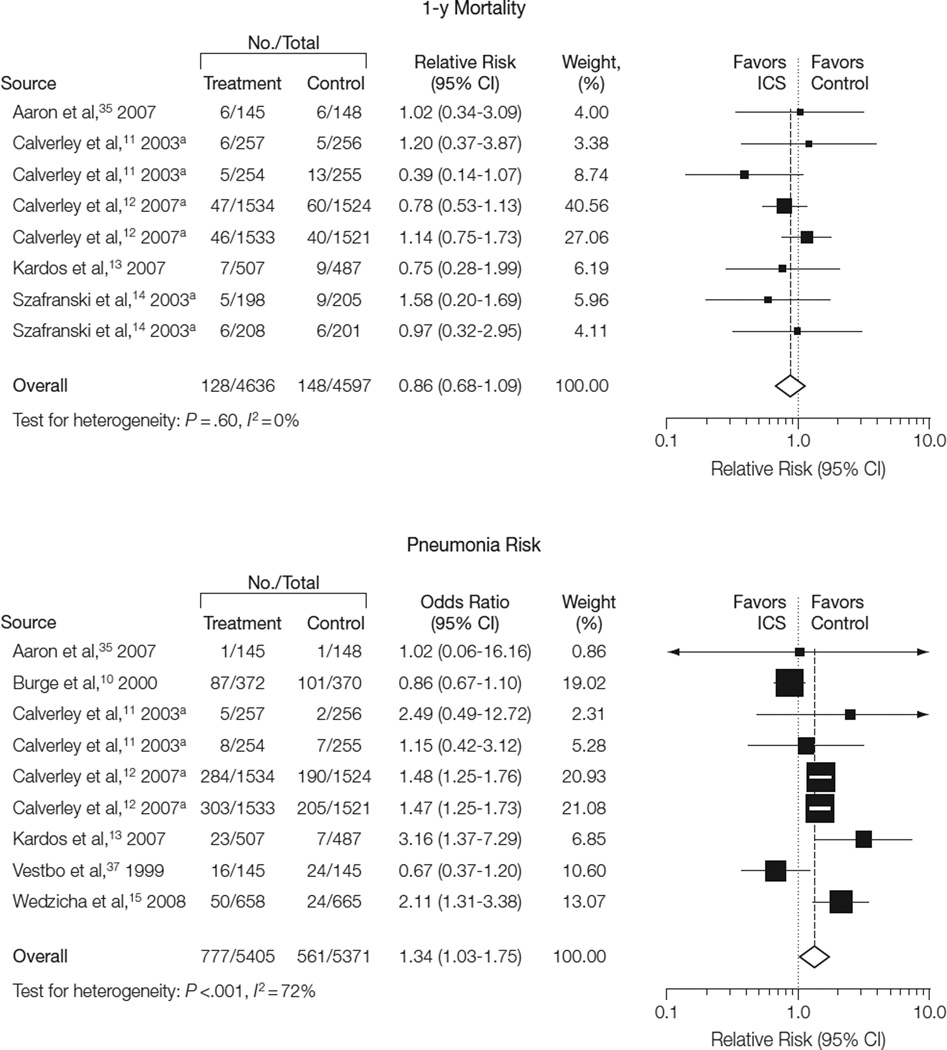
Results: Eleven eligible randomized controlled trials (14,426 participants) were included. In trials with mortality data, no difference was observed in 1-year all-cause mortality (128 deaths among 4636 patients in the treatment group and 148 deaths among 4597 patients in the control group; relative risk [RR], 0.86; 95% confidence interval [CI], 0.68-1.09; P = .20; I(2) = 0%). In the trials with data on pneumonia, ICS therapy was associated with a significantly higher incidence of pneumonia (777 cases among 5405 patients in the treatment group and 561 cases among 5371 patients in the control group; RR, 1.34; 95% CI, 1.03-1.75; P = .03; I(2) = 72%). Subgroup analyses indicated an increased risk of pneumonia in the following subgroups: highest ICS dose (RR, 1.46; 95% CI, 1.10-1.92; P = .008; I(2) = 78%), shorter duration of ICS use (RR, 2.12; 95% CI, 1.47-3.05; P < .001; I(2) = 0%), lowest baseline forced expiratory volume in the first second of expiration (RR, 1.90; 95% CI, 1.26-2.85; P = .002; I(2) = 0%), and combined ICS and bronchodilator therapy (RR, 1.57; 95% CI, 1.35-1.82; P < .001; I(2) = 24%).
Conclusions: Among patients with COPD, ICS therapy does not affect 1-year all-cause mortality. ICS therapy is associated with a higher risk of pneumonia. Future studies should determine whether specific subsets of patients with COPD benefit from ICS therapy.
Conflict of interest statement
Figures
Comment in
-
ACP Journal Club. Review: Inhaled corticosteroids do not reduce mortality but increase pneumonia in chronic obstructive pulmonary disease.Ann Intern Med. 2009 Mar 17;150(6):JC3-6. doi: 10.7326/0003-4819-150-6-200903170-02006. Ann Intern Med. 2009. PMID: 19306488 No abstract available.
-
Inhaled corticosteroids in patients with chronic obstructive pulmonary disease.JAMA. 2009 Apr 8;301(14):1432-3; author reply 1433-4. doi: 10.1001/jama.2009.436. JAMA. 2009. PMID: 19351933 No abstract available.
-
Inhaled corticosteroids in patients with chronic obstructive pulmonary disease.JAMA. 2009 Apr 8;301(14):1432; author reply 1433-4. doi: 10.1001/jama.2009.435. JAMA. 2009. PMID: 19351934 No abstract available.
-
Inhaled corticosteroids in patients with chronic obstructive pulmonary disease.JAMA. 2009 Apr 8;301(14):1433; author reply 1433-4. doi: 10.1001/jama.2009.437. JAMA. 2009. PMID: 19351935 No abstract available.
-
Review: inhaled corticosteroids do not reduce mortality but increase pneumonia in COPD.Evid Based Med. 2009 Jun;14(3):74. doi: 10.1136/ebm.14.3.74. Evid Based Med. 2009. PMID: 19483023 No abstract available.
-
Review: inhaled corticosteroids do not reduce mortality but increase pneumonia in chronic obstructive pulmonary disease.Evid Based Nurs. 2009 Jul;12(3):76. doi: 10.1136/ebn.12.3.76. Evid Based Nurs. 2009. PMID: 19553413 No abstract available.
References
-
- Jemal A, Ward E, Hao Y, Thun M. Trends in the leading causes of death in the United States, 1970–2002. JAMA. 2005;294(10):1255–1259. - PubMed
-
- Heron MP, Smith BL. Deaths: leading causes for 2003. Natl Vital Stat Rep. 2007;55:1–92. - PubMed
-
- Nocturnal Oxygen Therapy Trial Group. Continuous or nocturnal oxygen therapy in hypoxemic chronic obstructive lung disease: a clinical trial. Ann Intern Med. 1980;93(3):391–398. - PubMed
-
- Medical Research Council Working Party. Long term domiciliary oxygen therapy in chronic hypoxic cor pulmonale complicating chronic bronchitis and emphysema: report of the Medical Research Council Working Party. Lancet. 1981;1(8222):681–686. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
