

Comparison of fetal and neonatal growth curves in detecting growth restriction
- PMID: 19037030
- PMCID: PMC2752730
- DOI: 10.1097/AOG.0b013e31818bdc7e
Comparison of fetal and neonatal growth curves in detecting growth restriction
Abstract
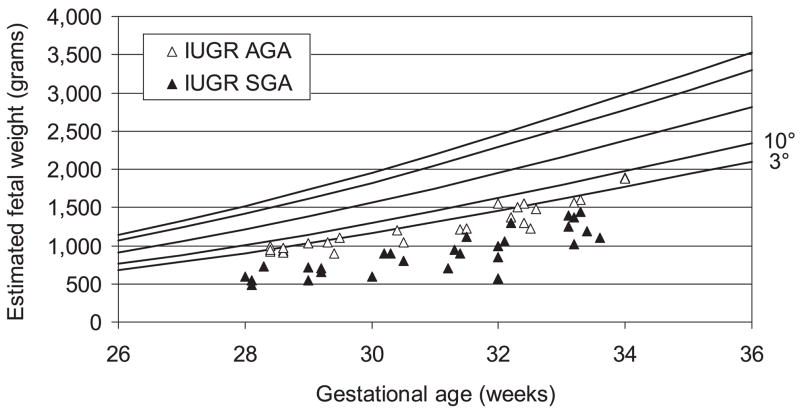
Objective: To evaluate the outcome of intrauterine growth restriction (IUGR) infants with abnormal pulsatility index of the umbilical artery according to the neonatal birth weight/gestational age standards and the intrauterine growth charts.
Methods: We analyzed 53 pregnancies with severe IUGR classified as group 2 (22 IUGR: abnormal pulsatility index and normal fetal heart rate) and group 3 (31 IUGR: abnormal pulsatility index and fetal heart rate). Neonatal birth weight/gestational age distribution, body size measurements, maternal characteristics and obstetric outcome, and neonatal major and minor morbidity and mortality were compared with those obtained in 79 singleton pregnancies with normal fetal growth and pulsatility index, matched for gestational age (appropriate for gestational age [AGA] group). Differences were analyzed with the chi(2) test and the Student t test. Differences between means corrected for gestational age in the different groups were assessed by analysis of covariance test. A P<.05 was considered significant.
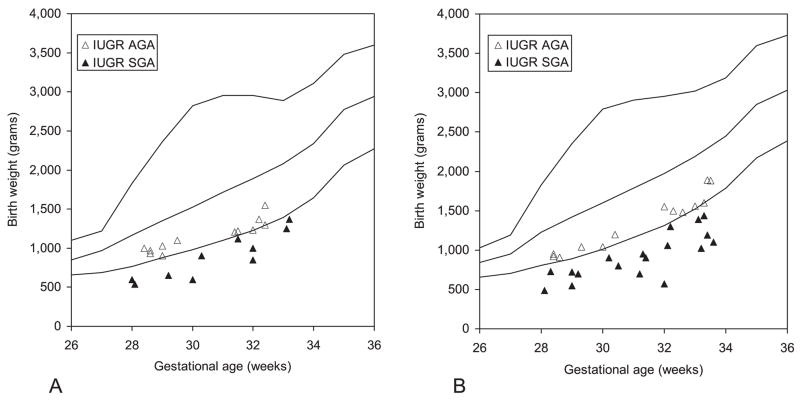
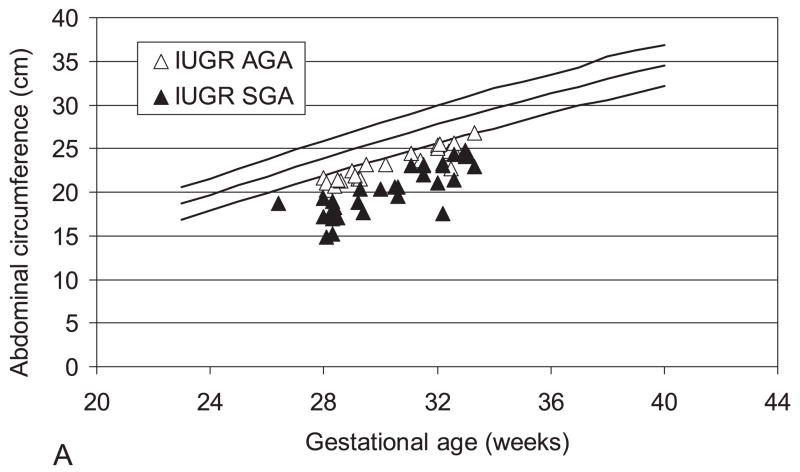
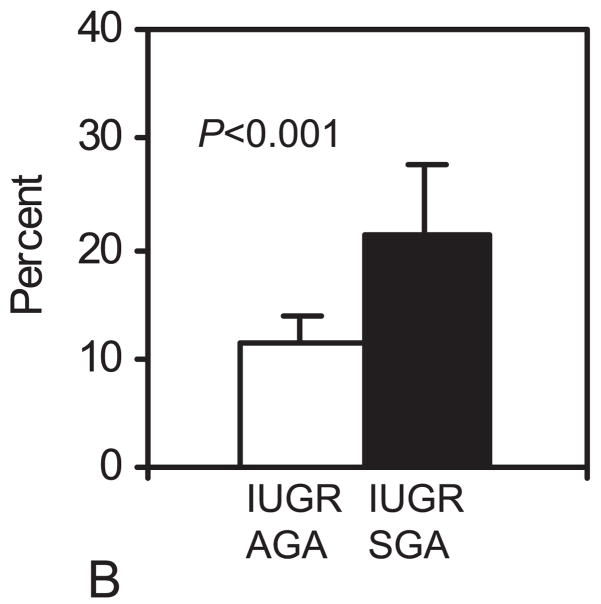
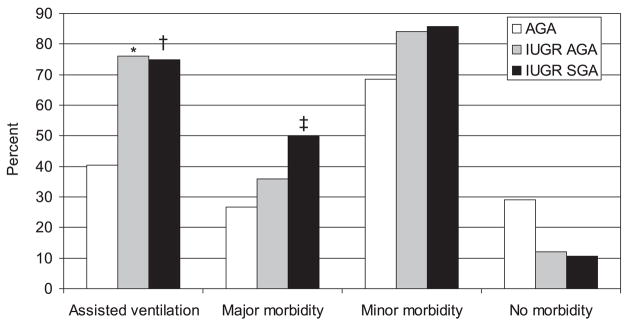
Results: At delivery, using the neonatal standards, 25 of 53 (47%) IUGR showed a birth weight above the 10th percentile (IUGR(AGA)), whereas in 28, birth weight was below the 10th percentile (IUGR small for gestational age [SGA]-IUGR(SGA)). All body size measurements were significantly higher in AGA than in IUGR(AGA) and IUGR(SGA). Forty-nine of 79 (62%) AGA and 49 of 53 (92%) IUGR were admitted to the neonatal intensive care unit (P<.001). One of 79 (1%) AGA and 6 of 53 (11%) IUGR newborns died within 28 days (P<.02). Major and minor morbidity was not different.
Conclusion: This study shows that neonatal outcome is similar in IUGR of the same clinical severity, whether or not they could be defined AGA or SGA according to the neonatal standards. Neonatal curves are misleading in detecting low birth weight infants and should be used only when obstetric data are unavailable.
Level of evidence: II.
Figures
Similar articles
-
Third-trimester growth diversity in small fetuses classified as appropriate-for-gestational age or small-for-gestational age at birth.Ultrasound Obstet Gynecol. 2021 Dec;58(6):882-891. doi: 10.1002/uog.23688. Ultrasound Obstet Gynecol. 2021. PMID: 33998089
-
Fetal growth restriction and intra-uterine growth restriction: guidelines for clinical practice from the French College of Gynaecologists and Obstetricians.Eur J Obstet Gynecol Reprod Biol. 2015 Oct;193:10-8. doi: 10.1016/j.ejogrb.2015.06.021. Epub 2015 Jul 2. Eur J Obstet Gynecol Reprod Biol. 2015. PMID: 26207980
-
Maternal serum ferritin as a clinical tool at 34-36 weeks' gestation for distinguishing subgroups of fetal growth restriction.J Matern Fetal Neonatal Med. 2017 Feb;30(4):452-456. doi: 10.1080/14767058.2016.1174997. Epub 2016 Apr 28. J Matern Fetal Neonatal Med. 2017. PMID: 27049175
-
Association of Intrauterine Growth Restriction and Small for Gestational Age Status With Childhood Cognitive Outcomes: A Systematic Review and Meta-analysis.JAMA Pediatr. 2020 Aug 1;174(8):772-781. doi: 10.1001/jamapediatrics.2020.1097. JAMA Pediatr. 2020. PMID: 32453414 Free PMC article.
-
Intrauterine growth restriction - part 2.J Matern Fetal Neonatal Med. 2016 Dec;29(24):4037-48. doi: 10.3109/14767058.2016.1154525. Epub 2016 Mar 15. J Matern Fetal Neonatal Med. 2016. PMID: 26979578 Review.
Cited by
-
Approaching the diagnosis of growth-restricted neonates: a cohort study.BMC Pregnancy Childbirth. 2010 Feb 1;10:6. doi: 10.1186/1471-2393-10-6. BMC Pregnancy Childbirth. 2010. PMID: 20122167 Free PMC article.
-
The Relationship Between Fetal Growth and Retinal Nerve Fiber Layer Thickness in a Cohort of Young Adults.Transl Vis Sci Technol. 2022 Jul 8;11(7):8. doi: 10.1167/tvst.11.7.8. Transl Vis Sci Technol. 2022. PMID: 35819290 Free PMC article.
-
Lung function between 8 and 15 years of age in very preterm infants with fetal growth restriction.Pediatr Res. 2021 Sep;90(3):657-663. doi: 10.1038/s41390-020-01299-0. Epub 2021 Jan 19. Pediatr Res. 2021. PMID: 33469172
-
Fetal growth velocity standards from the Fetal Growth Longitudinal Study of the INTERGROWTH-21st Project.Am J Obstet Gynecol. 2021 Feb;224(2):208.e1-208.e18. doi: 10.1016/j.ajog.2020.07.054. Epub 2020 Aug 5. Am J Obstet Gynecol. 2021. PMID: 32768431 Free PMC article.
-
Intrauterine growth restriction and its associated factors in South Gondar zone hospitals, Northwest Ethiopia, 2019.Arch Public Health. 2020 Sep 29;78:89. doi: 10.1186/s13690-020-00475-2. eCollection 2020. Arch Public Health. 2020. PMID: 33005403 Free PMC article.
References
-
- McIntire DD, Bloom SL, Casey BM, Leveno KJ. Birth weight in relation to morbidity and mortality among newborn infants. N Engl J Med. 1999;340:1234–8. - PubMed
-
- Piper JM, Xenakis EM, McFarland M, Elliott BD, Berkus MD, Langer O. Do growth-retarded premature infants have different rates of perinatal morbidity and mortality than appropriately grown premature infants? Obstet Gynecol. 1996;87:169–74. - PubMed
-
- Garite TJ, Clark R, Thorp JA. Intrauterine growth restriction increases morbidity and mortality among premature neonates. Am J Obstet Gynecol. 2004;191:481–7. - PubMed
-
- Bukowski R. Fetal growth potential and pregnancy outcome. Semin Perinatol. 2004;28:51–58. - PubMed
-
- Pardi G, Marconi AM, Cetin I, Lanfranchi A, Bozzetti P, Ferrazzi E, et al. Diagnostic value of blood sampling in fetuses with growth retardation. New Engl J Med. 1993;328:692–696. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
