

The course and outcome of unilateral intracranial arteriopathy in 79 children with ischaemic stroke
- PMID: 19039009
- PMCID: PMC2640213
- DOI: 10.1093/brain/awn313
The course and outcome of unilateral intracranial arteriopathy in 79 children with ischaemic stroke
Abstract
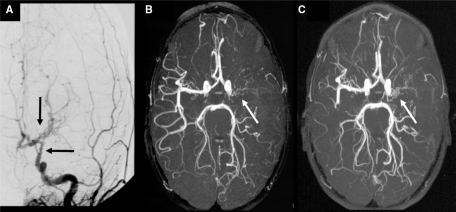
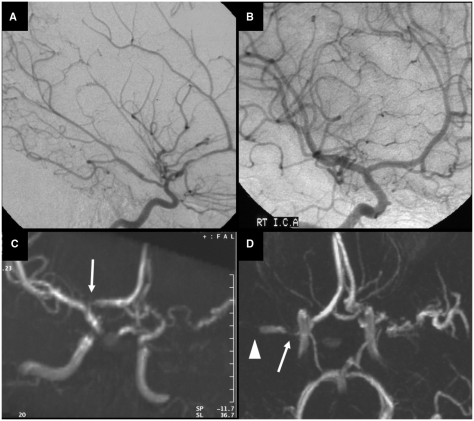
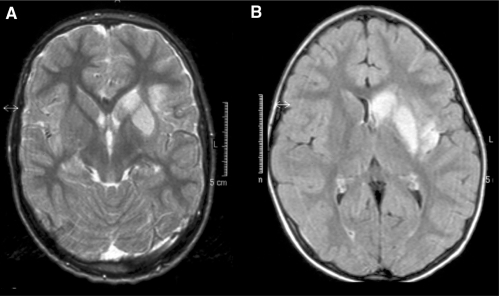
Arteriopathies are the commonest cause of arterial ischaemic stroke (AIS) in children. Repeated vascular imaging in children with AIS demonstrated the existence of a 'transient cerebral arteriopathy' (TCA), characterized by lenticulostriate infarction due to non-progressive unilateral arterial disease affecting the supraclinoid internal carotid artery and its proximal branches. To further characterize the course of childhood arteriopathies, and to differentiate TCA from progressive arterial disease, we studied the long-term evolution of unilateral anterior circulation arteriopathy, and explored predictors of stroke outcome and recurrence. From three consecutive cohorts in London, Paris and Utrecht, we reviewed radiological studies and clinical charts of 79 previously healthy children with anterior circulation AIS and unilateral intracranial arteriopathy of the internal carotid bifurcation, who underwent repeated vascular imaging. The long-term evolution of arteriopathy was classified as progressive or TCA. Clinical and imaging characteristics were compared between both groups. Logistic regression modelling was used to determine possible predictors of the course of arteriopathy, functional outcome and recurrence. After a median follow-up of 1.4 years, 5 of 79 children (6%) had progressive arteriopathy, with increasing unilateral disease or bilateral involvement. In the others (94%), the course of arteriopathy was classified as TCA. In 23% of TCA patients, follow-up vascular imaging showed complete normalization, the remaining 77% had residual arterial abnormalities, with improvement in 45% and stabilization in 32%. Stroke was preceded by chickenpox in 44% of TCA patients, and in none of the patients with progressive arteriopathies. Most infarcts were localized in the basal ganglia. In 14 (19%) of TCA patients, transient worsening of the arterial lesion was demonstrated before the arteriopathy stabilized or improved. Thirteen TCA patients (18%) had a recurrent stroke or TIA. Thirty TCA patients (41%) had a good neurological outcome, compared with none of the five patients with progressive arteriopathy. Arterial occlusion, moyamoya vessels and ACA involvement were more frequent in progressive arteriopathies. Cortical infarct localization was significantly associated with poor neurological outcome (OR 6.14, 95% CI 1.29-29.22, P = 0.02), while there was a trend for occlusive arterial disease to predict poor outcome (OR 3.00, 95% CI 0.98-9.23, P = 0.06). Progressive arteriopathy was associated with recurrence (OR 18.77, 95%CI 1.94-181.97, P = 0.01). The majority of childhood unilateral intracranial anterior circulation arteriopathies (94%) have a course that is consistent with TCA, in which transient worsening is common. Although the arterial inflammation probably causing TCA is 'transient', most children are left with permanent arterial abnormalities and residual neurological deficits.
Figures
References
-
- Askalan R, Laughlin S, Mayank S, Chan A, MacGregor D, Andrew M, et al. Chickenpox and stroke in childhood: a study of frequency and causation. Stroke. 2001;32:1257–62. - PubMed
-
- Benseler SM, deVeber G, Hawkins C, Schneider R, Tyrrell PN, Aviv RI, et al. Angiography-negative primary central nervous system vasculitis in children: a newly recognized inflammatory central nervous system disease. Arthritis Rheum. 2005;52:2159–67. - PubMed
-
- Benseler SM, Silverman E, Aviv RI, Schneider R, Armstrong D, Tyrrell PN, et al. Primary central nervous system vasculitis in children. Arthritis Rheum. 2006;54:1291–7. - PubMed
-
- Berger TM, Caduff JH, Gebbers JO. Fatal varicella-zoster virus antigen-positive giant cell arteritis of the central nervous system. Pediatr Infect Dis J. 2000;19:653–6. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
