

Interventional management of gastrointestinal fistulas
- PMID: 19039271
- PMCID: PMC2627247
- DOI: 10.3348/kjr.2008.9.6.541
Interventional management of gastrointestinal fistulas
Abstract
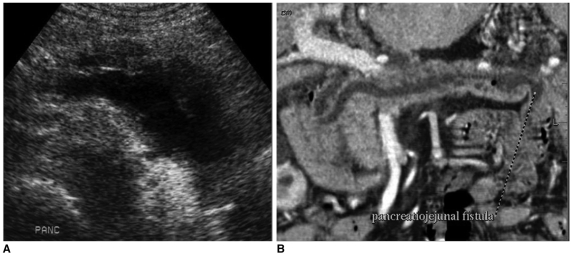
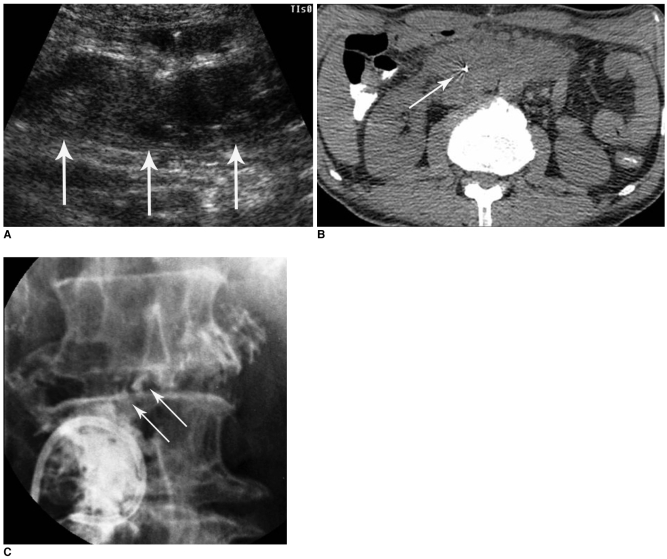
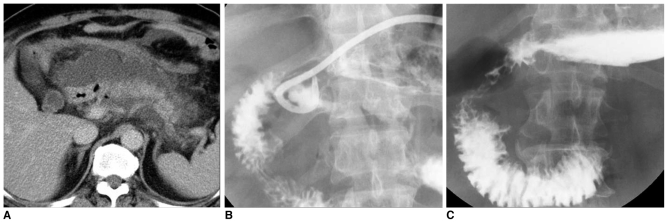
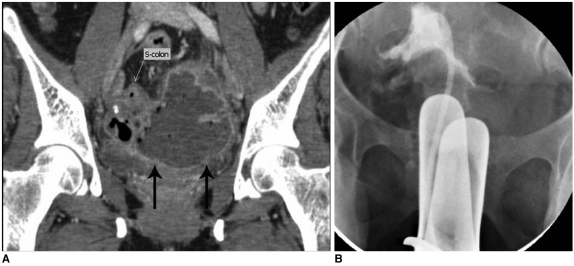
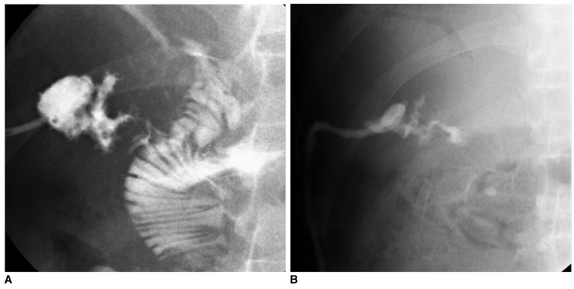
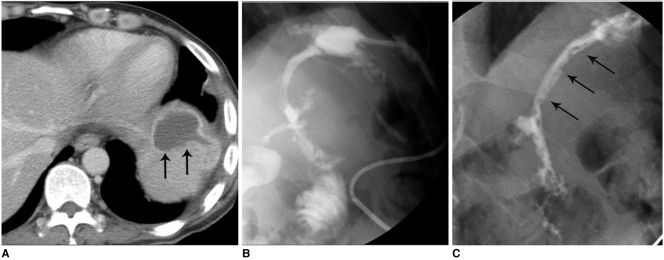
Gastrointestinal (GI) fistulas are frequently very serious complications that are associated with high morbidity and mortality. GI fistulas can cause a wide array of pathophysiological effects by allowing abnormal diversion of the GI contents, including digestive fluid, water, electrolytes, and nutrients, from either one intestine to another or from the intestine to the skin. As an alternative to surgery, recent technical advances in interventional radiology and percutaneous techniques have been shown as advantageous to lower the morbidity and mortality rate, and allow for superior accessibility to the fistulous tracts via the use of fistulography. In addition, new interventional management techniques continue to emerge. We describe the clinical and imaging features of GI fistulas and outline the interventional management of GI fistulas.
Figures
References
-
- McLean GK, Mackie JA, Freiman DB, Ring EJ. Enterocutaneous fistulae: interventional radiologic management. AJR Am J Roentgenol. 1982;138:615–619. - PubMed
-
- Boverie JH, Remont A. Percutaneous management of fistulas in the digestive tract. In: Dondelinger RF, Rossi P, Kurdziel JC, Wallace S, editors. Interventional radiology. Stuttgart: Thieme; 1990. pp. 746–753.
-
- Berry SM, Fischer JE. Classification and pathophysiology of enterocutaneous fistulas. Surg Clin North Am. 1996;76:1009–1018. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
