

The involvement of human amnion in histologic chorioamnionitis is an indicator that a fetal and an intra-amniotic inflammatory response is more likely and severe: clinical implications
- PMID: 19046766
- PMCID: PMC4136806
- DOI: 10.1016/j.placenta.2008.09.017
The involvement of human amnion in histologic chorioamnionitis is an indicator that a fetal and an intra-amniotic inflammatory response is more likely and severe: clinical implications
Abstract
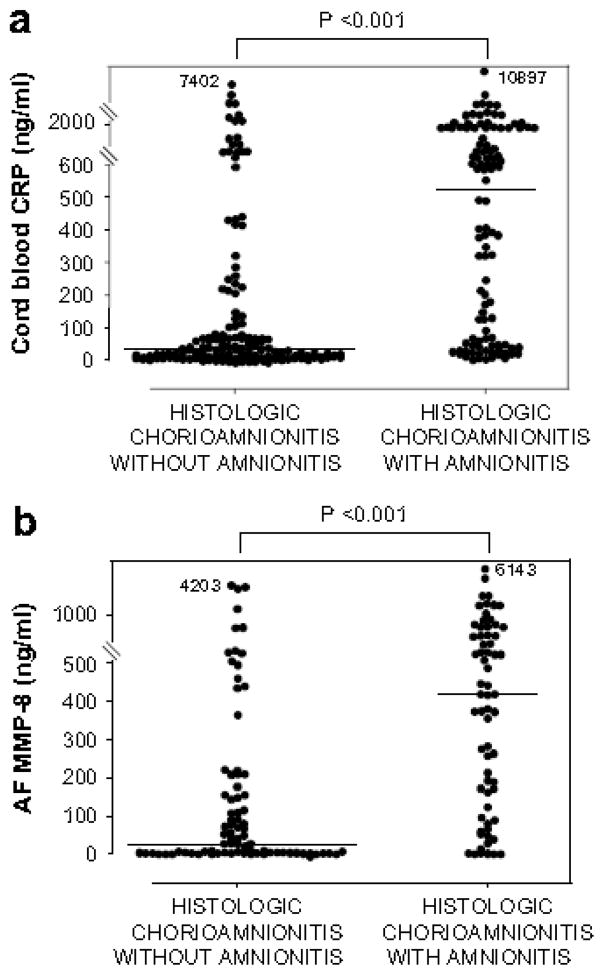
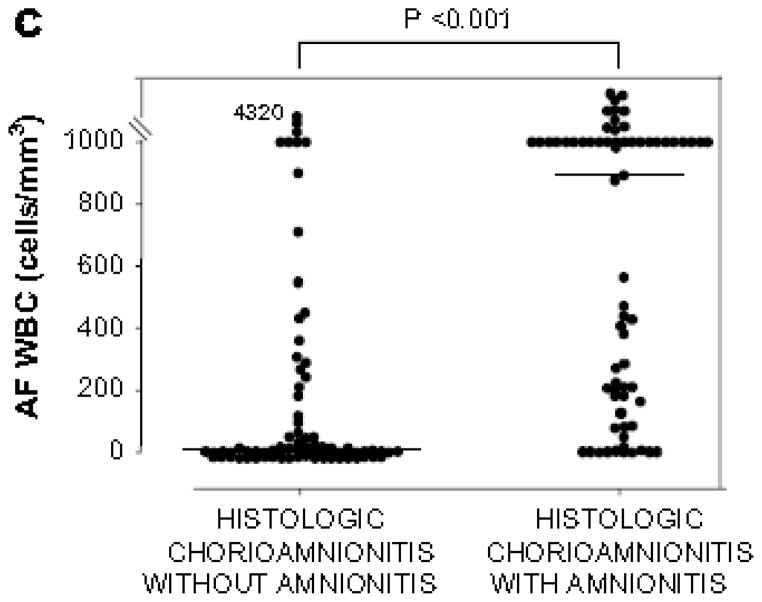
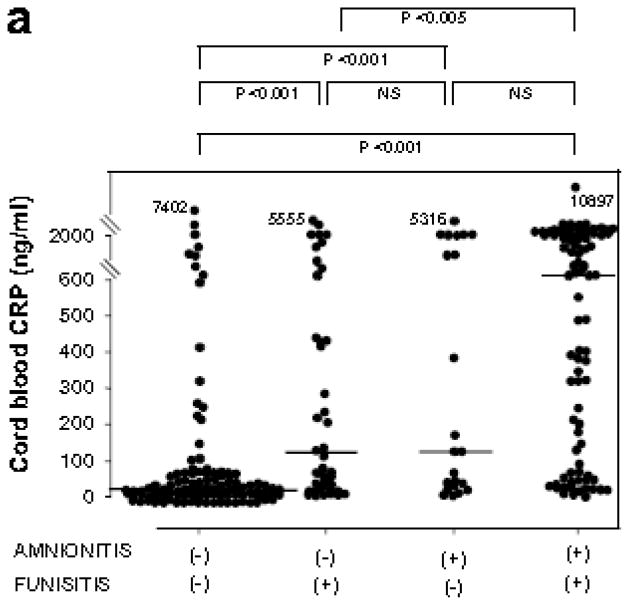
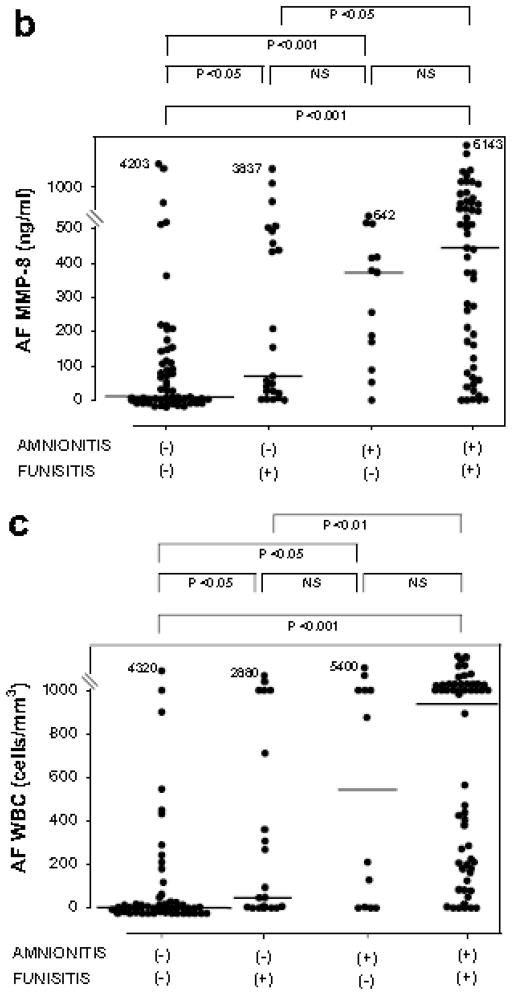
Objective: Amnionitis (inflammation of the amnion) is the final stage of extra-placental chorioamniotic inflammation. We propose that patients with "amnionitis", rather than "chorionitis" have a more advanced form of intra-uterine inflammation/infection and, thus, would have a more intense fetal and intra-amniotic inflammatory response than those without "amnionitis".
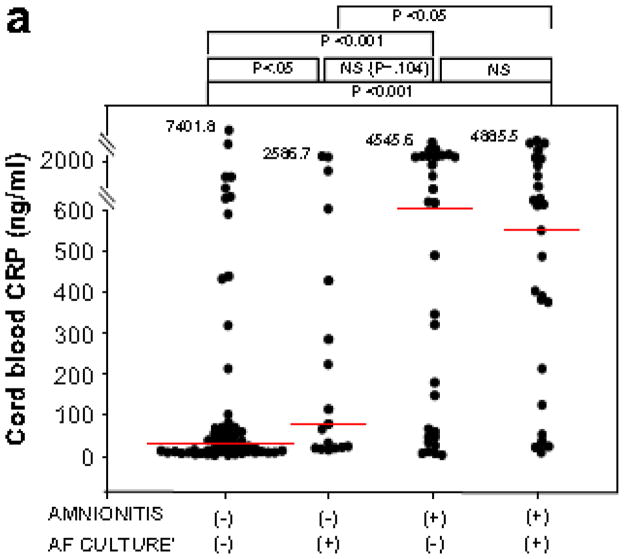
Study design: The relationship between the presence of amnionitis, and a fetal and an intra-amniotic inflammatory response was examined in 290 singleton preterm births (<or=36 weeks) with histologic chorioamnionitis. The fetal inflammatory response was determined by plasma C-reactive protein (CRP) concentrations in umbilical cord and the presence of funisitis. The intra-amniotic inflammatory response was assessed by matrix metalloproteinase-8 (MMP-8) concentration and white blood cell (WBC) count in 156 amniotic fluid (AF) samples obtained within 5 days of birth. AF was cultured for aerobic and anaerobic bacteria and genital mycoplasmas. The CRP concentration was measured with a highly sensitive immunoassay.
Results: (1) Amnionitis was present in 43.1% of cases with histologic chorioamnionitis. (2) Patients with amnionitis had a significantly higher rate of funisitis and positive AF culture and a higher median umbilical cord plasma CRP, AF MMP-8 level and AF WBC count than those without amnionitis (p<0.001 for each). (3) Among cases with amnionitis, the presence or absence of funisitis was not associated with significant differences in the median cord plasma CRP, AF MMP-8 level and AF WBC count. (4) However, the presence of amnionitis in cases with funisitis was associated with a higher median umbilical cord plasma CRP, AF MMP-8 level and AF WBC count than the absence of amnionitis in those with funisitis (p<0.05 for each). (5) Multiple logistic regression analysis demonstrated that amnionitis was a better independent predictor of proven or suspected early-onset neonatal sepsis (odds ratio 3.8, 95% confidence interval (CI) 1.1-13.2, p<0.05) than funisitis (odds ratio 1.8, 95% CI 0.5-6.1, not significant) after correction for the contribution of other potential confounding variables.
Conclusion: The involvement of the amnion in the inflammatory process of the extraplacental membranes is associated with a more intense fetal and intra-amniotic inflammatory response than chorionitis alone. This observation has clinical implications because it allows staging of the severity of the inflammatory process and assessment of the likelihood of fetal involvement.
Figures

References
-
- Bobitt JR, Hayslip CC, Damato JD. Amniotic fluid infection as determined by transabdominal amniocentesis in patients with intact membranes in premature labor. Am J Obstet Gynecol. 1981;140:947–52. - PubMed
-
- Hameed C, Tejani N, Verma UL, Archbald F. Silent chorioamnionitis as a cause of preterm labor refractory to tocolytic therapy. Am J Obstet Gynecol. 1984;149:726–30. - PubMed
-
- Wahbeh CJ, Hill GB, Eden RD, Gall SA. Intra-amniotic bacterial colonization in premature labor. Am J Obstet Gynecol. 1984;148:739–43. - PubMed
-
- Gravett MG, Hummel D, Eschenbach DA, Holmes KK. Preterm labor associated with subclinical amniotic fluid infection and with bacterial vaginosis. Obstet Gynecol. 1986;67:229–37. - PubMed
-
- Leigh J, Garite TJ. Amniocentesis and the management of premature labor. Obstet Gynecol. 1986;67:500–6. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
