

Chemokine markers predict biochemical recurrence of prostate cancer following prostatectomy
- PMID: 19047106
- PMCID: PMC3050736
- DOI: 10.1158/1078-0432.CCR-08-1716
Chemokine markers predict biochemical recurrence of prostate cancer following prostatectomy
Abstract
Purpose: Stratifying patients who have a high risk of prostate cancer recurrence following prostatectomy can potentiate the use of adjuvant therapy at an early stage. Inflammation has emerged as a mediator of prostate cancer metastatic progression. We hypothesized that chemokines can be biomarkers for distinguishing patients with high risk for biochemical recurrence of prostate cancer.
Experimental design: In a nested case-control study, 82 subjects developed biochemical recurrence within 5 years of prostatectomy. Prostate tissues from 98 age-matched subjects who were recurrence-free following prostatectomy in the same period were the controls. A high-throughput lectin-based enrichment of prostate tissue enabled multiplex ELISA to identify the expression of three chemokines to discriminate the two patient populations.
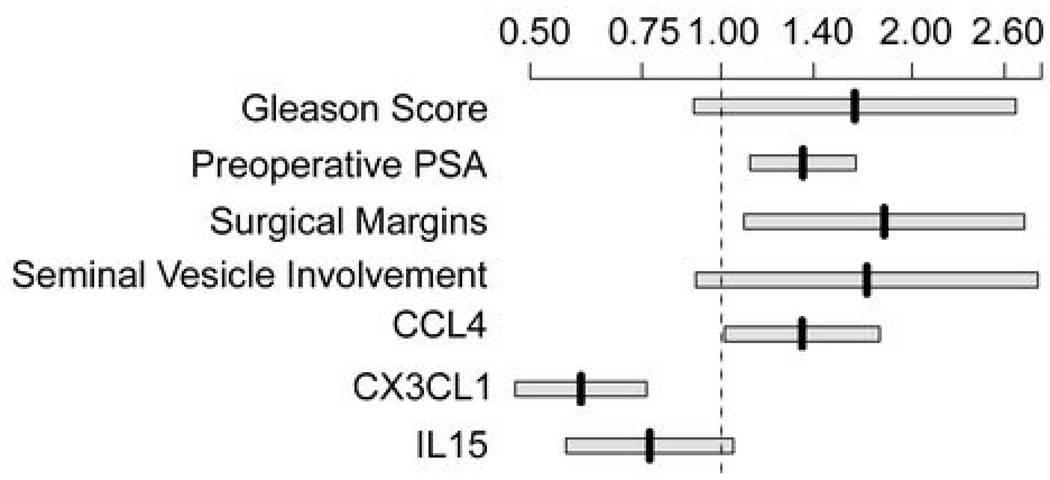
Results: The expression of CX3CL1 and IL-15 in prostate tissue was associated with 5-year biochemical recurrence-free survival following prostatectomy. However, the expression of chemokine ligand 4 (CCL4) was associated with biochemical recurrence. Multivariable logistic regression model combining preoperative prostate-specific antigen, Gleason score, surgical margin, and seminal vesicle status with the three chemokines doubled the specificity of prediction at 90% sensitivity compared with use of the clinicopathologic variables alone (P < 0.0001). Survival analysis yielded a nomogram that supported the use of CX3CL1, IL-15, and CCL4 in predicting 1-, 3-, and 5-year recurrence-free survival after prostatectomy.
Conclusions: Each of the three chemokines can serve as independent predictors of biochemical recurrence. However, the combination of chemokine biomarkers plus clinicopathologic variables discriminated prostatectomy subjects for the probability of biochemical recurrence significantly better than clinicopathologic variables alone.
Figures




References
-
- Jemal A, Tiwari RC, Murray T, et al. Cancer statistics, 2004. CA Cancer J Clin. 2004;54:8–29. - PubMed
-
- Thompson KE, Hernandez J, Canby-Hagino ED, Troyer D, Thompson IM. Prognostic features in men who died of prostate cancer. J Urol. 2005;174:553–556. discussion 6. - PubMed
-
- Glode LM. The case for adjuvant therapy for prostate cancer. J Urol. 2006;176:S30–S33. - PubMed
-
- Gomella LG, Zeltser I, Valicenti RK. Use of neoadjuvant and adjuvant therapy to prevent or delay recurrence of prostate cancer in patients undergoing surgical treatment for prostate cancer. Urology. 2003;62 Suppl 1:46–54. - PubMed
-
- Akduman B, Crawford ED. The management of high risk prostate cancer. J Urol. 2003;169:1993–1998. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
