

Genomic imbalances in neonates with birth defects: high detection rates by using chromosomal microarray analysis
- PMID: 19047251
- PMCID: PMC2795566
- DOI: 10.1542/peds.2008-0297
Genomic imbalances in neonates with birth defects: high detection rates by using chromosomal microarray analysis
Abstract
Objectives: Our aim was to determine the frequency of genomic imbalances in neonates with birth defects by using targeted array-based comparative genomic hybridization, also known as chromosomal microarray analysis.
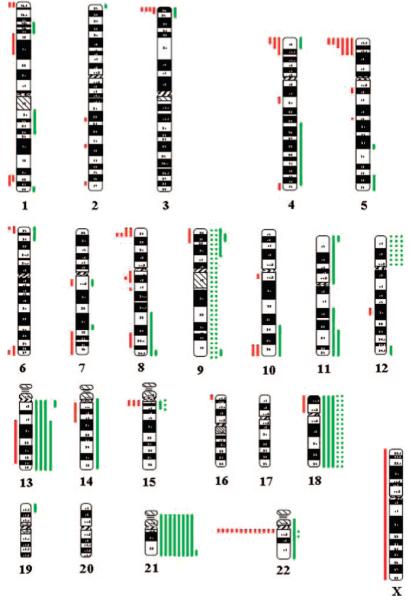
Methods: Between March 2006 and September 2007, 638 neonates with various birth defects were referred for chromosomal microarray analysis. Three consecutive chromosomal microarray analysis versions were used: bacterial artificial chromosome-based versions V5 and V6 and bacterial artificial chromosome emulated oligonucleotide-based version V6 Oligo. Each version had targeted but increasingly extensive genomic coverage and interrogated>150 disease loci with enhanced coverage in genomic rearrangement-prone pericentromeric and subtelomeric regions.
Results: Overall, 109 (17.1%) patients were identified with clinically significant abnormalities with detection rates of 13.7%, 16.6%, and 19.9% on V5, V6, and V6 Oligo, respectively. The majority of these abnormalities would not be defined by using karyotype analysis. The clinically significant detection rates by use of chromosomal microarray analysis for various clinical indications were 66.7% for "possible chromosomal abnormality"+/-"others" (other clinical indications), 33.3% for ambiguous genitalia+/-others, 27.1% for dysmorphic features+multiple congenital anomalies+/-others, 24.6% for dysmorphic features+/-others, 21.8% for congenital heart disease+/-others, 17.9% for multiple congenital anomalies+/-others, and 9.5% for the patients referred for others that were different from the groups defined. In all, 16 (2.5%) patients had chromosomal aneuploidies, and 81 (12.7%) patients had segmental aneusomies including common microdeletion or microduplication syndromes and other genomic disorders. Chromosomal mosaicism was found in 12 (1.9%) neonates.
Conclusions: Chromosomal microarray analysis is a valuable clinical diagnostic tool that allows precise and rapid identification of genomic imbalances and mosaic abnormalities as the cause of birth defects in neonates. Chromosomal microarray analysis allows for timely molecular diagnoses and detects many more clinically relevant genomic abnormalities than conventional cytogenetic studies, enabling more informed decision-making and management and appropriate assessment of recurrence risk.
Figures
References
-
- Mathews TJ, MacDorman MF. Infant mortality statistics from the 2003 period linked birth/infant death data set. Natl Vital Stat Rep. 2006;54(16):1–29. - PubMed
-
- Canfield MA, Honein MA, Yuskiv N, et al. National estimates and race/ethnic-specific variation of selected birth defects in the United States, 1999–2001. Birth Defects Res A Clin Mol Teratol. 2006;76(11):747–756. - PubMed
-
- Hamerton JL, Canning N, Ray M, Smith S. A cytogenetic survey of 14,069 newborn infants: I—incidence of chromosome abnormalities. Clin Genet. 1975;8(4):223–243. - PubMed
-
- Evans JA, de von FR, Greenberg C, Ramsay S, Hamerton JL. A cytogenetic survey of 14,069 newborn infants: IV—further follow-up on the children with sex chromosome anomalies. Birth Defects Orig Artic Ser. 1982;18(4):169–184. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
