

Natural history of CNS relapse in patients with aggressive non-Hodgkin's lymphoma: a 20-year follow-up analysis of SWOG 8516 -- the Southwest Oncology Group
- PMID: 19047289
- PMCID: PMC4879698
- DOI: 10.1200/JCO.2008.16.8021
Natural history of CNS relapse in patients with aggressive non-Hodgkin's lymphoma: a 20-year follow-up analysis of SWOG 8516 -- the Southwest Oncology Group
Abstract
Purpose: To investigate the incidence, natural history, and risk factors predictive of CNS relapse in patients with de novo aggressive lymphomas and to evaluate the efficacy of CNS prophylaxis in patients with initial bone marrow (BM) involvement.
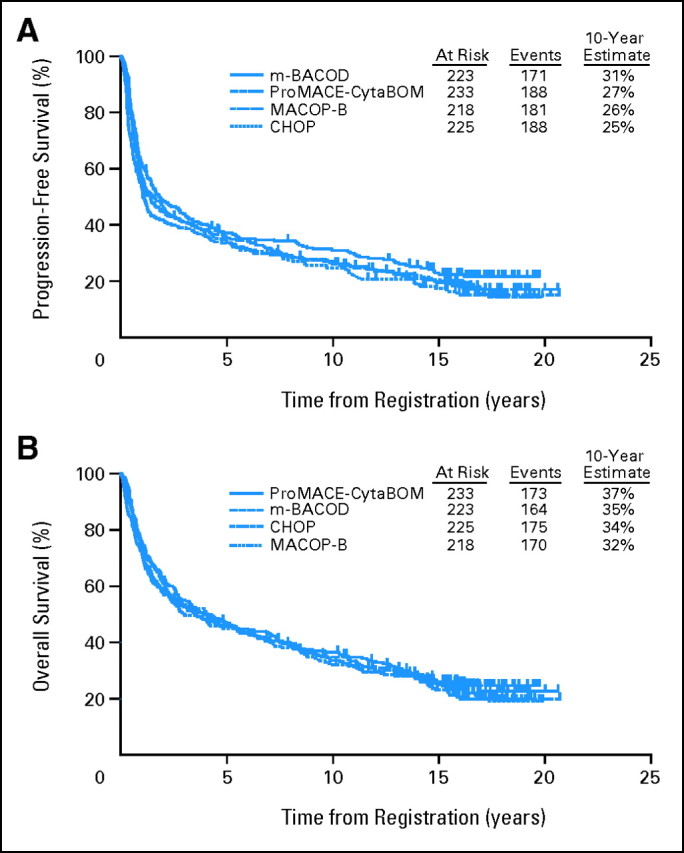
Patients and methods: We conducted an analysis of CNS events from 20-year follow-up data on 899 eligible patients with aggressive lymphoma treated on Southwest Oncology Group protocol 8516, a randomized trial of CHOP (cyclophosphamide, doxorubicin, vincristine, prednisone), MACOP-B (methotrexate, doxorubicin, cyclophosphamide, vincristine, prednisone, and bleomycin), ProMACE (prednisone, methotrexate, doxorubicin, cyclophosphamide, etoposide)-CytaBOM (cytarabine, bleomycin, vincristine, methotrexate), and m-BACOD (methotrexate, bleomycin, cyclophosphamide, etoposide). Patients with BM involvement randomly assigned to receive ProMACE-CytaBOM (63 patients) or m-BACOD (58 patients) were to receive CNS prophylaxis, whereas those randomly assigned to receive CHOP or MACOP-B did not.
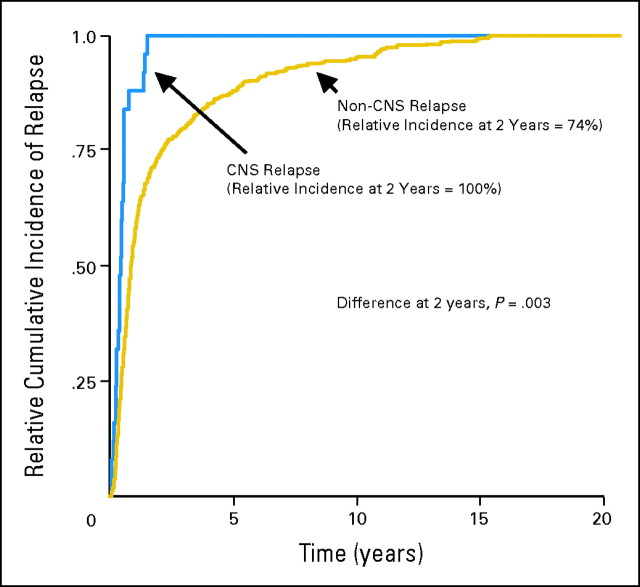
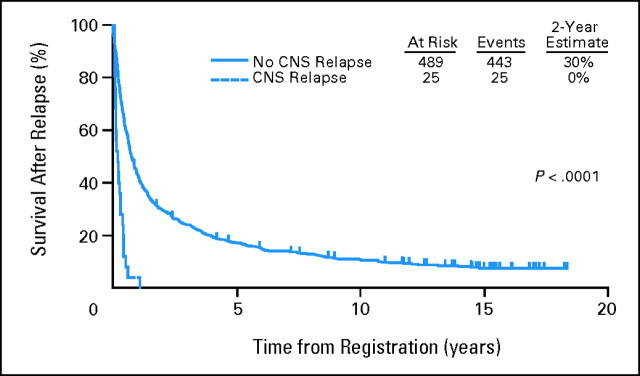
Results: CNS relapse is uncommon (25 of 899 patients), with a cumulative incidence of 2.8%. CNS relapse occurs early (median time to relapse, 5.4 months from diagnosis). Indeed, 20 of 25 patients with CNS relapse relapsed during chemotherapy, or within 6 months of completion. The number of extranodal sites and the International Prognostic Index were predictive of CNS relapse. There was no significant benefit of CNS prophylaxis in patients with BM involvement at diagnosis; however, given the small number of events, the power of this analysis is limited.
Conclusion: The early occurrence of CNS events suggests that these patients had subclinical disease at initial diagnosis. As such, strategies to better detect and treat patients with subclinical CNS disease at diagnosis would be anticipated to result in a decrease in the incidence of CNS relapse, without subjecting those patients not destined for CNS relapse to unnecessary and potentially toxic prophylaxis strategies.
Figures
Comment in
-
Natural History of CNS Relapse in Aggressive Non-Hodgkin's Lymphoma: What Have We Learned?J Clin Oncol. 2009 Jul 20;27(21):e26; author reply e27-8. doi: 10.1200/JCO.2009.22.0608. Epub 2009 Jun 22. J Clin Oncol. 2009. PMID: 19546401 No abstract available.
References
-
- Sparling HJ, Adams R, Parker F Jr: Involvement of the nervous system by malignant lymphoma. Medicine 26:285-332, 1947 - PubMed
-
- Bunn PA Jr, Schein PS, Banks PM, et al: Central nervous system complications in patients with diffuse histiocytic and undifferentiated lymphoma: Leukemia revisited. Blood 47:3-10, 1976 - PubMed
-
- Litam JP, Cabanillas F, Smith TL, et al: Central nervous system relapse in malignant lymphomas: Risk factors and implications for prophylaxis. Blood 54:1249-1257, 1979 - PubMed
-
- Herman TS, Hammond N, Jones SE, et al: Involvement of the central nervous system by non-Hodgkin's lymphoma: The Southwest Oncology Group experience. Cancer 43:390-397, 1979 - PubMed
-
- Law IP, Dick FR, Blom J, et al: Involvement of the central nervous system in non-Hodgkin's lymphoma. Cancer 36:225-231, 1975 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
