

Randomized trial of reamed and unreamed intramedullary nailing of tibial shaft fractures
- PMID: 19047701
- PMCID: PMC2663330
- DOI: 10.2106/JBJS.G.01694
Randomized trial of reamed and unreamed intramedullary nailing of tibial shaft fractures
Abstract
Background: There remains a compelling biological rationale for both reamed and unreamed intramedullary nailing for the treatment of tibial shaft fractures. Previous small trials have left the evidence for either approach inconclusive. We compared reamed and unreamed intramedullary nailing with regard to the rates of reoperations and complications in patients with tibial shaft fractures.
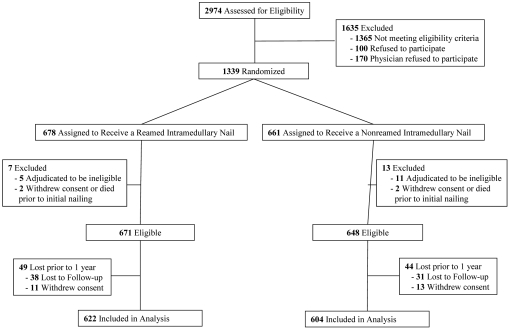
Methods: We conducted a multicenter, blinded randomized trial of 1319 adults in whom a tibial shaft fracture was treated with either reamed or unreamed intramedullary nailing. Perioperative care was standardized, and reoperations for nonunion before six months were disallowed. The primary composite outcome measured at twelve months postoperatively included bone-grafting, implant exchange, and dynamization in patients with a fracture gap of <1 cm. Infection and fasciotomy were considered as part of the composite outcome, irrespective of the postoperative gap.
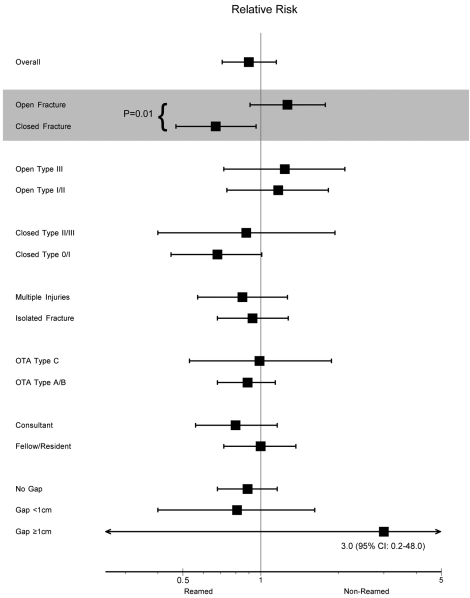
Results: One thousand two hundred and twenty-six participants (93%) completed one year of follow-up. Of these, 622 patients were randomized to reamed nailing and 604 patients were randomized to unreamed nailing. Among all patients, fifty-seven (4.6%) required implant exchange or bone-grafting because of nonunion. Among all patients, 105 in the reamed nailing group and 114 in the unreamed nailing group experienced a primary outcome event (relative risk, 0.90; 95% confidence interval, 0.71 to 1.15). In patients with closed fractures, forty-five (11%) of 416 in the reamed nailing group and sixty-eight (17%) of 410 in the unreamed nailing group experienced a primary event (relative risk, 0.67; 95% confidence interval, 0.47 to 0.96; p = 0.03). This difference was largely due to differences in dynamization. In patients with open fractures, sixty of 206 in the reamed nailing group and forty-six of 194 in the unreamed nailing group experienced a primary event (relative risk, 1.27; 95% confidence interval, 0.91 to 1.78; p = 0.16).
Conclusions: The present study demonstrates a possible benefit for reamed intramedullary nailing in patients with closed fractures. We found no difference between approaches in patients with open fractures. Delaying reoperation for nonunion for at least six months may substantially decrease the need for reoperation.
Figures
Comment in
-
Randomized trial of reamed and unreamed intramedullary nailing of tibial shaft fractures.J Bone Joint Surg Am. 2009 May;91(5):1274; author reply 1274-5. J Bone Joint Surg Am. 2009. PMID: 19411479 No abstract available.
References
-
- Russell TA. Fractures of the tibial diaphysis. In: Levine AM, ed. Orthopaedic knowledge update: trauma. Vol 1. Rosemont IL: American Academy of Orthopaedic Surgeons; 1996. p 171-9.
-
- Bhandari M, Guyatt GH, Swiontkowski MF, Schemitsch EH. Treatment of open fractures of the shaft of the tibia. J Bone Joint Surg Br. 2001;83:62-8. - PubMed
-
- Bhandari M, Guyatt GH, Tong D, Adili A, Shaughnessy SG. Reamed versus nonreamed intramedullary nailing of lower extremity long bone fractures: a systematic overview and meta-analysis. J Orthop Trauma. 2000;14:2-9. - PubMed
-
- Forster MC, Bruce AS, Aster AS. Should the tibia be reamed when nailing? Injury. 2005;36:439-44. - PubMed
-
- Rhinelander FW. Tibial blood supply in relation to fracture healing. Clin Orthop Relat Res. 1974;105:34-81. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
