

Development history and concept of an oral anticancer agent S-1 (TS-1): its clinical usefulness and future vistas
- PMID: 19052037
- PMCID: PMC2639406
- DOI: 10.1093/jjco/hyn127
Development history and concept of an oral anticancer agent S-1 (TS-1): its clinical usefulness and future vistas
Abstract
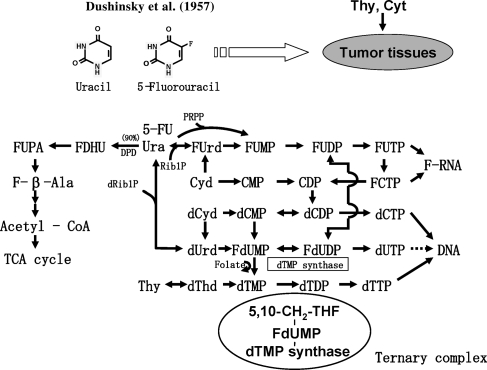
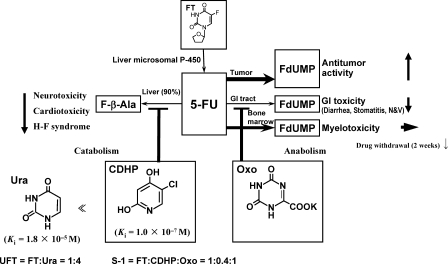
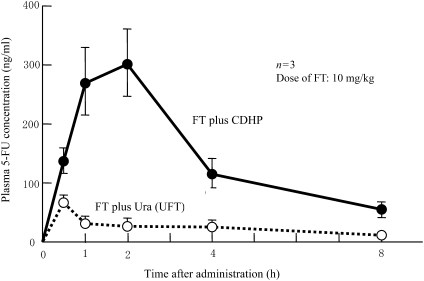
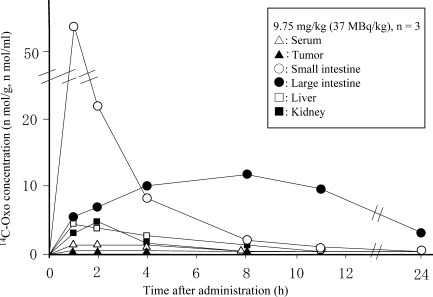
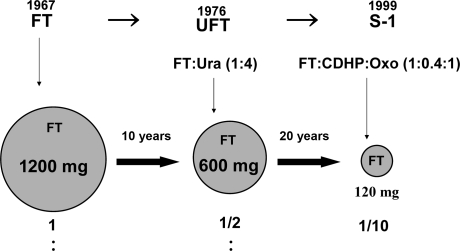
Dushinsky et al. left a great gift to human beings with the discovery of 5-fluorouracil (5-FU). Approximately 50 years have elapsed from that discovery to the development of S-1 (TS-1). The concept of developing an anticancer agent that simultaneously possesses both efficacy-enhancing and adverse reaction-reducing effects could be achieved only with a three-component combination drug. S-1 is an oral anticancer agent containing two biochemical modulators for 5-FU and tegafur (FT), a metabolically activated prodrug of 5-FU. The first modulator, 5-chloro-2,4-dihydroxypyridine (CDHP), enhances the pharmacological actions of 5-FU by potently inhibiting its degradation. The second modulator, potassium oxonate (Oxo), localizing in mucosal cells of the gastrointestinal (GI) tract after oral administration, reduces the incidence of GI toxicities by suppressing the activation of 5-FU in the GI tract. Thus, S-1 combines FT, CDHP and Oxo at a molar ratio of 1:0.4:1. In 1999-2007, S-1 was approved for the treatment of the following seven cancers: gastric, head and neck, colorectal, non-small cell lung, breast, pancreatic and biliary tract cancers. 'S-1 and low-dose cisplatin therapy' without provoking Grade 3 non-hematologic toxicities was proposed to enhance its clinical usefulness. Furthermore, 'alternate-day S-1 regimen' may improve the dosing schedule for 5-FU by utilizing its strongly time-dependent mode of action; the former is characterized by the low incidences of myelotoxicity and non-hematologic toxicities (e.g. < or =Grade 1 anorexia, fatigue, stomatitis, nausea, vomiting and taste alteration). These two approaches are considered to allow long-lasting therapy with S-1.
Figures
References
-
- Goodman LS, Wintrobe MM, Dameshek W, Goodman MJ, Gilman A, McLennan MT. Nitrogen mustard therapy. Use of methyl-bis(beta-chloroethyl) amine hydrochloride and tris (beta-chloroethyl)amine hydrochloride for Hodgkin’s disease, lymphosarcoma, leukemia, and certain allied and miscellaneous disorders. J Am Med Assoc. 1946;132:126–32. Reprinted in J Am Med Assoc 1984;251:2255-61. - PubMed
-
- Hata T, Sano R, Sugawara R, Matsumae A, Kanamori K, Shima T, et al. Mitomycin, a new antibiotic from Streptomyces. J Antib Ser A. 1956;9:141–6. - PubMed
-
- Dushinsky R, Pleven E, Heidelberger C. The synthesis of 5-fluoropyrimidines. J Am Chem Soc. 1957;79:4559–60.
-
- MacDonald JS, Schein P, Woolley PV, Smythe T, Ueno W, Hoth D, et al. 5-Fluorouracil, doxorubicin, and mitomycin (FAM) combination chemotherapy for advanced gastric cancer. Ann Intern Med. 1980;93:533–6. - PubMed
-
- Lokich JJ, Ahlgren JD, Gullo JJ, Philips JA, Fryer JG. A prospective randomized comparison of continuous infusion fluorouracil with conventional bolus schedule in metastatic colorectal carcinoma: A Mid-Atlantic Oncology Program Study. J Clin Oncol. 1989;7:425–32. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
