

Diagnosis of pediatric pulmonary tuberculosis by stool PCR
- PMID: 19052299
- PMCID: PMC2912504
Diagnosis of pediatric pulmonary tuberculosis by stool PCR
Abstract
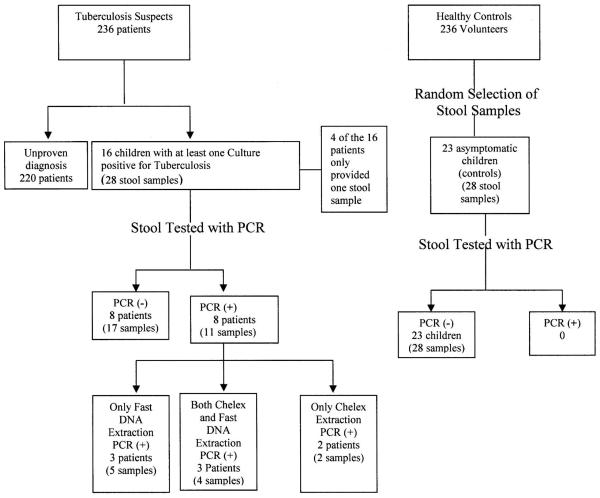
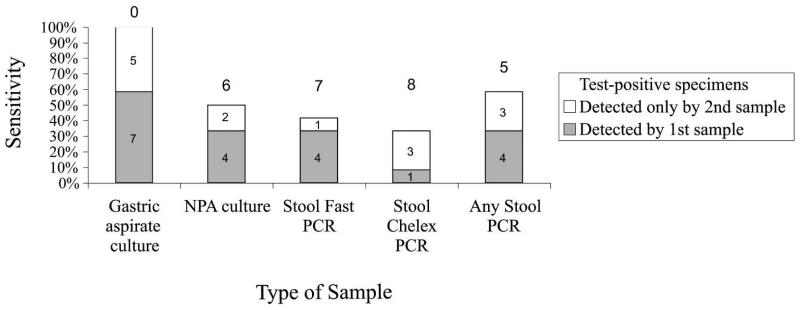
Pediatric pulmonary tuberculosis diagnosis is difficult because young children are unable to expectorate sputum samples. Testing stool for tuberculosis DNA from swallowed sputum may diagnose pulmonary tuberculosis. Hospitalized children with suspected tuberculosis had stool, nasopharyngeal, and gastric aspirates cultured that confirmed pulmonary tuberculosis in 16/236 patients. Twenty-eight stored stools from these 16 children were used to evaluate stool polymerase chain reaction (PCR) for tuberculosis diagnosis compared with 28 stool samples from 23 healthy control children. Two DNA extraction techniques were used: fast-DNA mechanical homogenization and Chelex-resin chemical extraction. DNA was tested for tuberculosis DNA with a hemi-nested IS6110 PCR. PCR after Fast-DNA processing was positive for 6/16 culture-proven tuberculosis patients versus 5/16 after Chelex extraction (sensitivity 38% and 31%, respectively). All controls were negative (specificity 100%). If sensitivity can be increased, stool PCR would be a rapid, non-invasive, and relatively bio-secure initial test for children with suspected pulmonary tuberculosis.
Figures
References
-
- WHO-WHO/TUB . Guidelines for Tuberculosis Treatment in Adults and Children in National Tuberculosis Programs. Tuberculosis Unit Division of Communicable Diseases. Third edition World Health Organization; Geneva: 2003.
-
- WHO . Tuberculosis. World Health Organization; Geneva: 1995. Fact sheet No. 93.
-
- Zar HJ, Hanslo D, Apolles P, Swingler G, Hussey G. Induced sputum versus gastric lavage for microbiological confirmation of pulmonary tuberculosis in infants and young children: a prospective study. Lancet. 2005;365:130–134. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical