

A novel interdisciplinary analgesic program reduces pain and improves function in older adults after orthopedic surgery
- PMID: 19054187
- PMCID: PMC2729399
- DOI: 10.1111/j.1532-5415.2008.02063.x
A novel interdisciplinary analgesic program reduces pain and improves function in older adults after orthopedic surgery
Abstract
Objectives: To examine the effect of a multicomponent intervention on pain and function after orthopedic surgery.
Design: Controlled prospective propensity score-matched clinical trial.
Setting: New York City acute rehabilitation hospital.
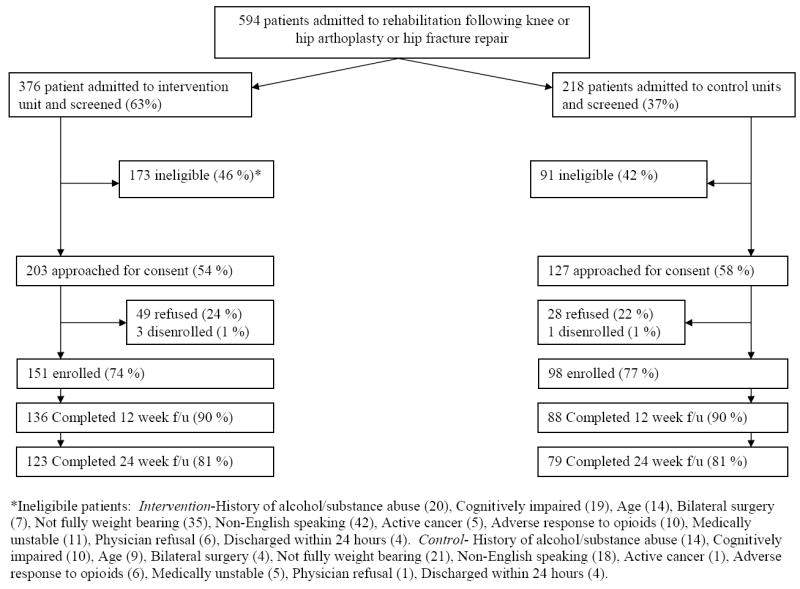
Participants: Two hundred forty-nine patients admitted to rehabilitation after hip fracture repair (n=51) or hip (n=64) or knee (n=134) arthroplasty.
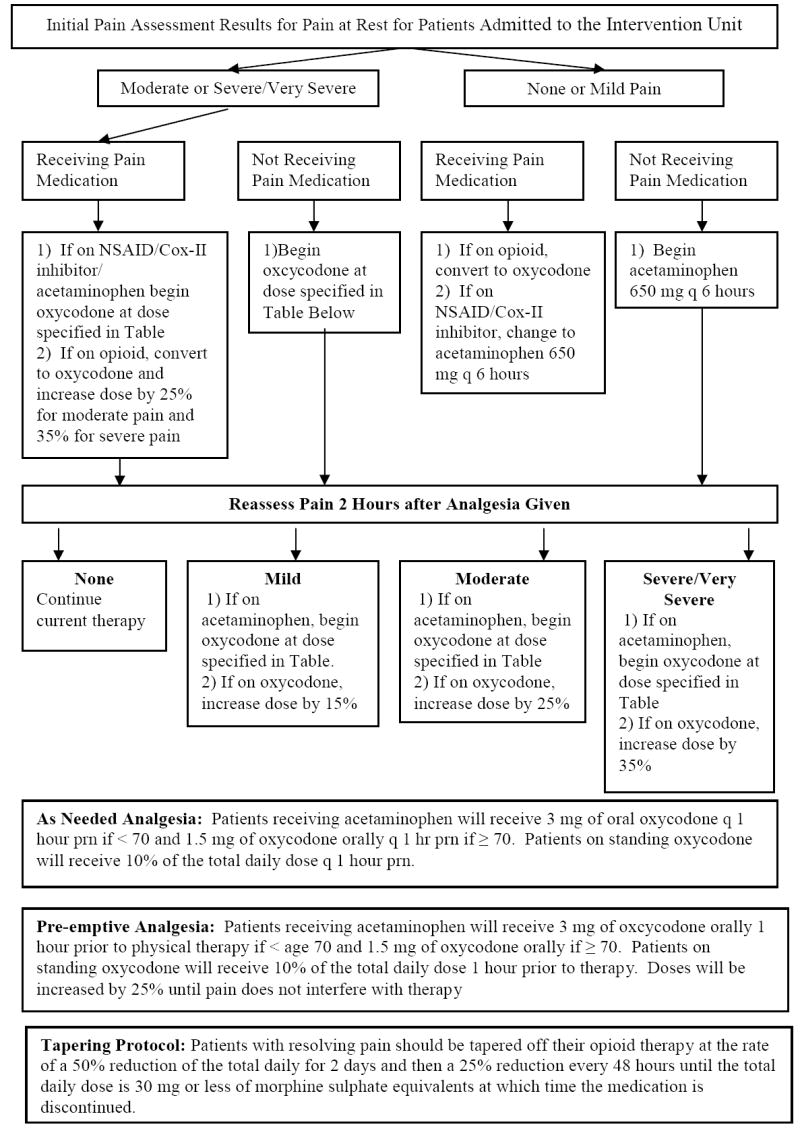
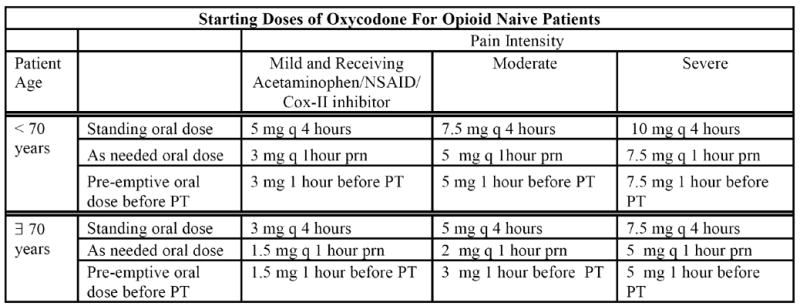
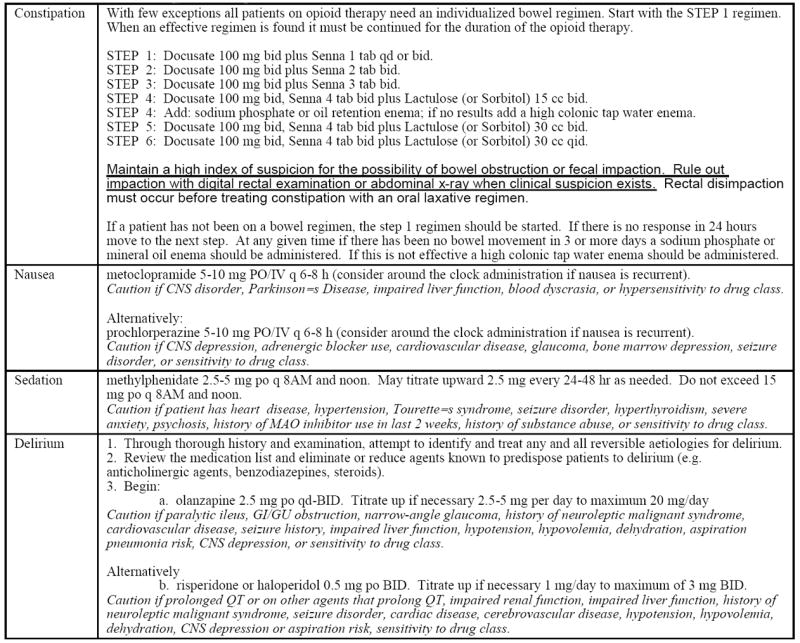
Intervention: Pain assessment at rest and with physical therapy (PT) by staff using numeric rating scales (1 to 5). Physician protocols for standing analgesia and preemptive analgesia before PT were implemented on the intervention unit. Control unit patients received usual care.
Measurements: Pain, analgesic prescribing, gait speed, transfer time, and percentage of PT sessions completed during admission. Pain and difficulty walking at 6, 12, 18, and 24 weeks after discharge.
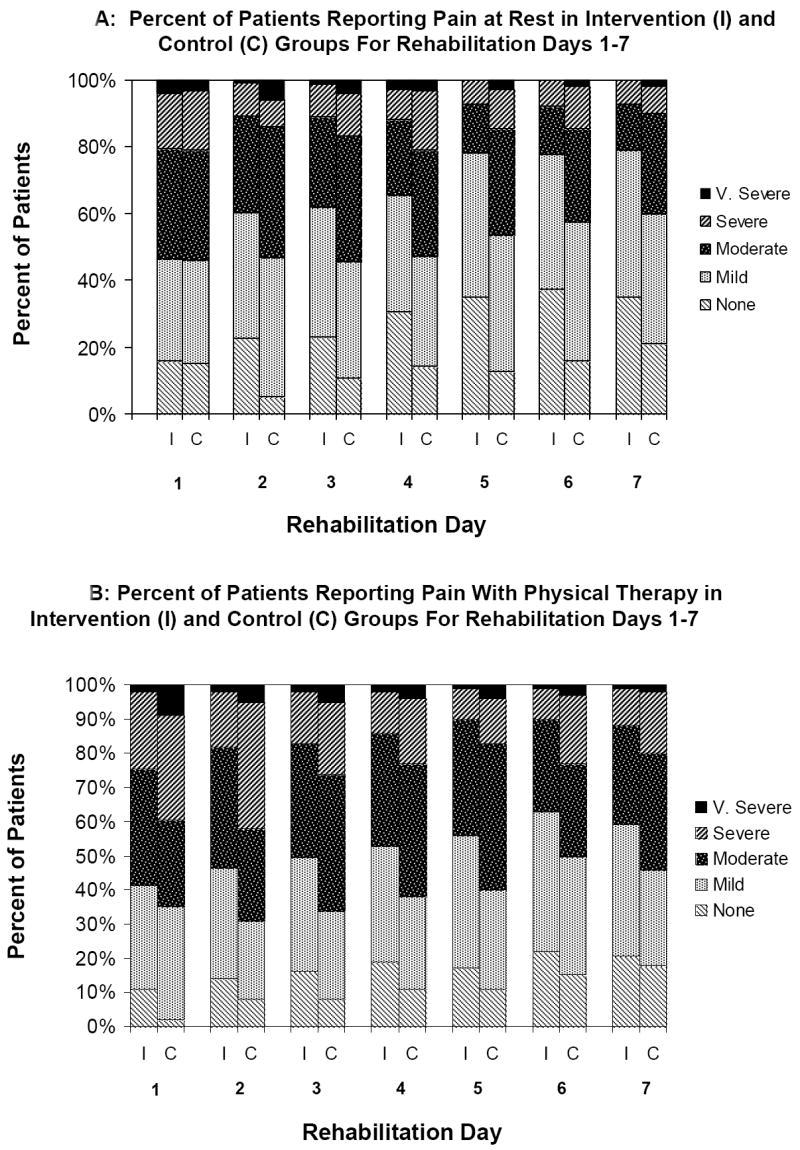
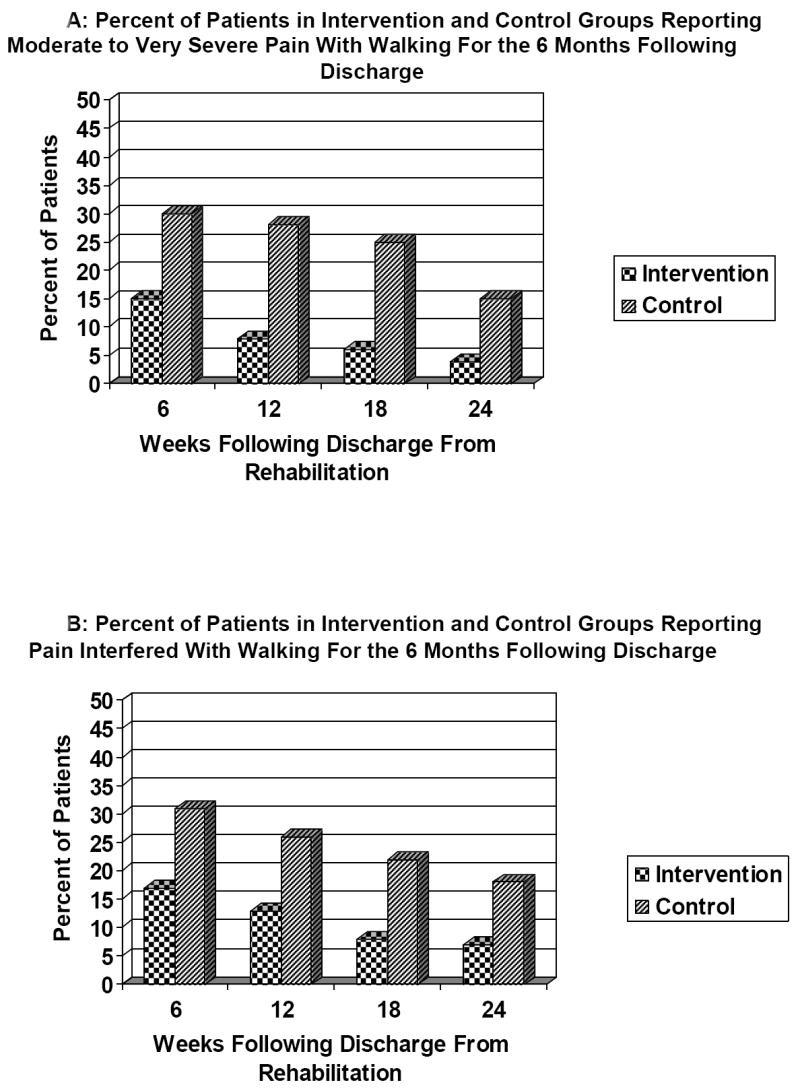
Results: In multivariable analyses intervention patients were significantly more likely than controls to report no or mild pain at rest (66% vs 49%, P=.004) and with PT (52% vs 38%, P=.02) on average for the first 7 days of rehabilitation, had faster 8-foot-walk times on Days 4 (9.3 seconds vs 13.2 seconds, P=.02) and 7 (6.9 vs 9.2 seconds, P=.02), received more analgesia (23.6 vs 15.6 mg of morphine sulfate equivalents per day, P<.001), were more likely to receive standing orders for analgesia (98% vs 48%, P<.001), and had significantly shorter lengths of stay (10.1 vs 11.3 days, P=.005). At 6 months, intervention patients were less likely than controls to report moderate to severe pain with walking (4% vs 15%, P=.02) and that pain did not interfere with walking (7% vs 18%, P=.004) and were less likely to be taking analgesics (35% vs 51%, P=.03).
Conclusion: The intervention improved postoperative pain, reduced chronic pain, and improved function.
Conflict of interest statement
Figures
Comment in
-
Novel interdisciplinary analgesic program.J Am Geriatr Soc. 2009 Aug;57(8):1505; author reply 1505-6. doi: 10.1111/j.1532-5415.2009.02358.x. J Am Geriatr Soc. 2009. PMID: 19682147 No abstract available.
References
-
- Goldberg GR, Morrison RS. Pain management in hospitalized cancer patients. J Clin Oncol. 2007;25:1792–801. - PubMed
-
- Max MB. How to move pain and symptom research from the margin to the mainstream. J Pain. 2003;4:355–360. - PubMed
-
- Munin MC, Kwoh CK, Glynn N, et al. Predicting discharge outcome after elective hip and knee arthroplasty. Am J Phys Med Rehabil. 1995;74:294–301. - PubMed
-
- Cheville A, Chen A, Oster G, et al. A randomized trial of controlled-release oxycodone during inpatient rehabilitation following unilateral total knee arthroplasty. J Bone Joint Surg Am. 2001;83-A:572–576. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
