

Efficacy and toxicity of methotrexate (MTX) monotherapy versus MTX combination therapy with non-biological disease-modifying antirheumatic drugs in rheumatoid arthritis: a systematic review and meta-analysis
- PMID: 19054823
- PMCID: PMC2689526
- DOI: 10.1136/ard.2008.099861
Efficacy and toxicity of methotrexate (MTX) monotherapy versus MTX combination therapy with non-biological disease-modifying antirheumatic drugs in rheumatoid arthritis: a systematic review and meta-analysis
Abstract
Objective: To evaluate the efficacy and toxicity of methotrexate (MTX) monotherapy compared with MTX combination with non-biological disease-modifying antirheumatic drugs (DMARDs) in adults with rheumatoid arthritis.
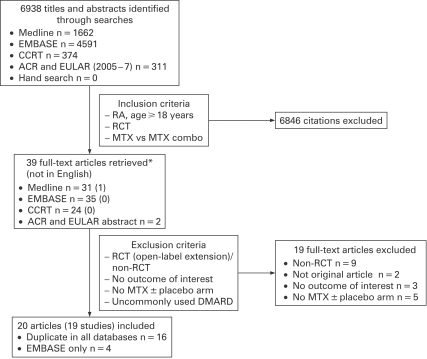
Method: A systematic review of randomised trials comparing MTX alone and in combination with other non-biological DMARDs was carried out. Trials were identified in Medline, EMBASE, the Cochrane Library and ACR/EULAR meeting abstracts. Primary outcomes were withdrawals for adverse events or lack of efficacy.
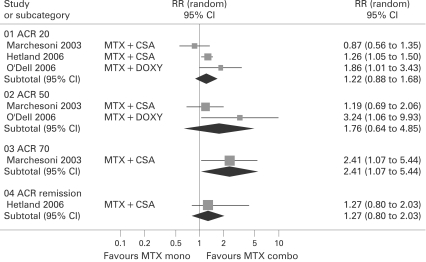
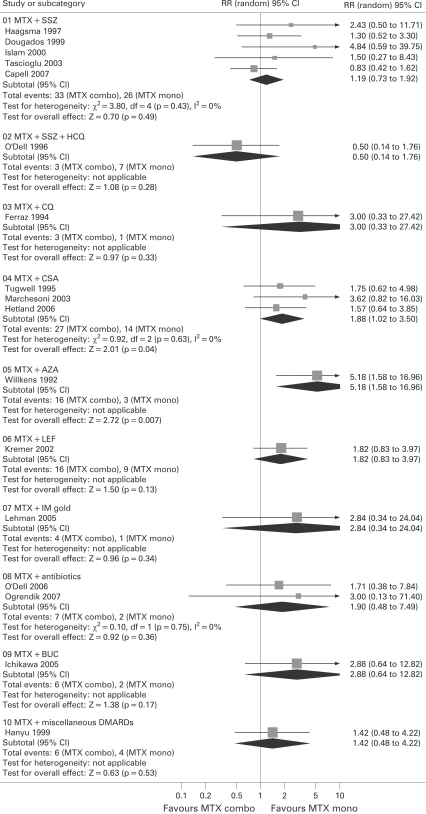
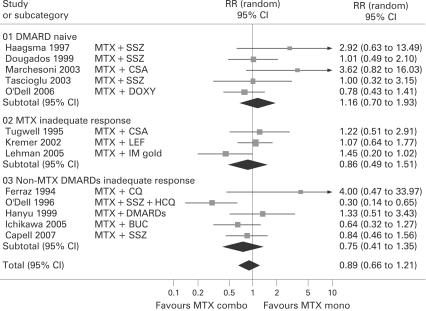
Results: A total of 19 trials (2025 patients) from 6938 citations were grouped by the type of patients randomised. Trials in DMARD naive patients showed no significant advantage of the MTX combination versus monotherapy; withdrawals for lack of efficacy or toxicity were similar in both groups (relative risk (RR) = 1.16; 95% CI 0.70 to 1.93). Trials in MTX or non-MTX DMARD inadequate responder patients also showed no difference in withdrawal rates between the MTX combo versus mono groups (RR = 0.86; 95% CI 0.49 to 1.51 and RR = 0.75; 95% CI 0.41 to 1.35), but in one study the specific combination of MTX with sulfasalazine and hydroxychloroquine showed a better efficacy/toxicity ratio than MTX alone with RR = 0.3 (95% CI 0.14 to 0.65). Adding leflunomide to MTX non-responders improved efficacy but increased the risk of gastrointestinal side effects and liver toxicity. Withdrawals for toxicity were most significant with ciclosporin and azathioprine combinations.
Conclusion: In DMARD naive patients the balance of efficacy/toxicity favours MTX monotherapy. In DMARD inadequate responders the evidence is inconclusive. Trials are needed that compare currently used MTX doses and combination therapies.
Conflict of interest statement
Figures


References
-
- Möttönen T, Hannonen P, Leirisalo-Repo M, Nissilä M, Kautiainen H, Korpela M, et al. Comparison of combination therapy with single-drug therapy in early rheumatoid arthritis: a randomised trial Lancet 1999;353:1568–73 - PubMed
-
- Goekoop-Ruiterman YPM, de Vries-Bouwstra J, Allaart C, van Zeben D, Kerstens PJSM, Hazes J, et al. Clinical and radiographic outcomes of four different treatment strategies in patients with early rheumatoid arthritis (the BeSt study): a randomized, controlled trial. Arthritis Rheum 2005;52:3381–90 - PubMed
-
- Goekoop-Ruiterman YPM, de Vries-Bouwstra J, Allaart C, van Zeben D, Kerstens PJSM, Hazes J, et al. Comparison of treatment strategies in early rheumatoid arthritis: a randomized trial. Ann Intern Med 2007;146:406–15 - PubMed
-
- Marchesoni A, Battafarano N, Arreghini M, Gallazzi M, Tosi S. Radiographic progression in early rheumatoid arthritis: a 12-month randomized controlled study comparing the combination of cyclosporin and methotrexate with methotrexate alone. Rheumatology (Oxford) 2003;42:1545–9 - PubMed
-
- Tascioglu F, Oner C, Armagan O. Comparison of low dose methotrexate and combination therapy with methotrexate and sulphasalazine in the treatment of early rheumatoid arthritis. J Rheumatol Med Rehab 2003;14:142–9
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
