

Tight perioperative glucose control is associated with a reduction in renal impairment and renal failure in non-diabetic cardiac surgical patients
- PMID: 19055829
- PMCID: PMC2646319
- DOI: 10.1186/cc7145
Tight perioperative glucose control is associated with a reduction in renal impairment and renal failure in non-diabetic cardiac surgical patients
Abstract
Introduction: Acute renal failure after cardiac surgery increases in-hospital mortality. We evaluated the effect of intra- and postoperative tight control of blood glucose levels on renal function after cardiac surgery based on the Risk, Injury, Failure, Loss, and End-stage kidney failure (RIFLE) criteria, and on the need for acute postoperative dialysis.
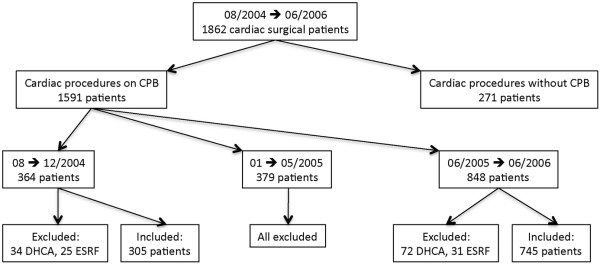
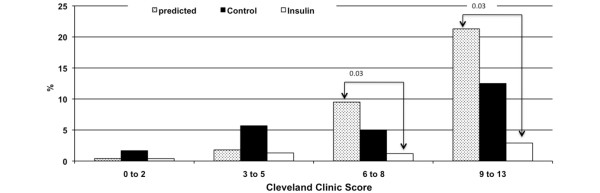
Methods: We retrospectively analyzed two groups of consecutive patients undergoing cardiac surgery with cardiopulmonary bypass between August 2004 and June 2006. In the first group, no tight glycemic control was implemented (Control, n = 305). Insulin therapy was initiated at blood glucose levels > 150 mg/dL. In the group with tight glycemic control (Insulin, n = 745), intra- and postoperative blood glucose levels were targeted between 80 to 110 mg/dL, using the Aalst Glycemia Insulin Protocol. Postoperative renal impairment or failure was evaluated with the RIFLE score, based on serum creatinine, glomerular filtration rate and/or urinary output. We used the Cleveland Clinic Severity Score to compare the predicted vs observed incidence of acute postoperative dialysis between groups.
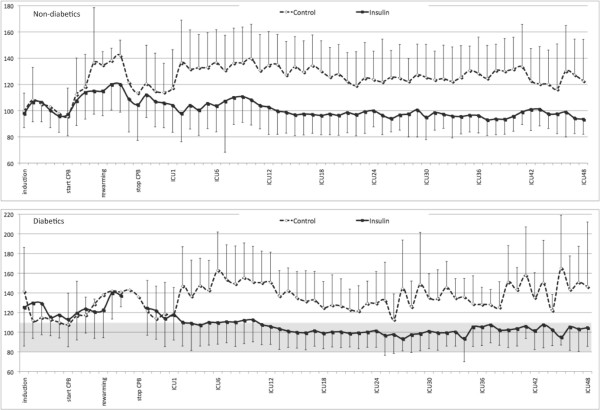
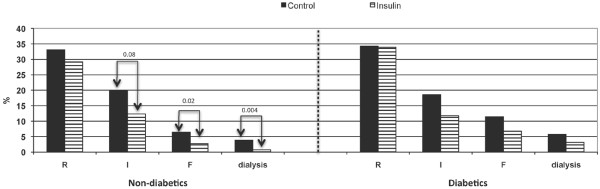
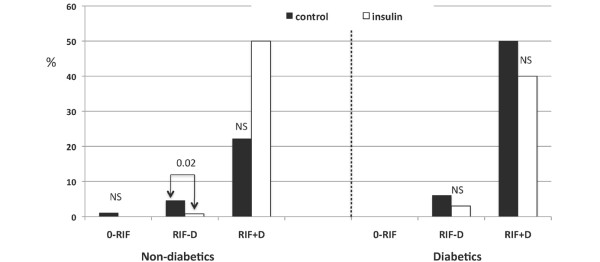
Results: Mean blood glucose levels in the Insulin group were lower compared to the Control group from rewarming on cardiopulmonary bypass onwards until ICU discharge (p < 0.0001). Median ICU stay was 2 days in both groups. In non-diabetics, strict perioperative blood glucose control was associated with a reduced incidence of renal impairment (p = 0.01) and failure (p = 0.02) scoring according to RIFLE criteria, as well as a reduced incidence of acute postoperative dialysis (from 3.9% in Control to 0.7% in Insulin; p < 0.01). The 30-day mortality was lower in the Insulin than in the Control group (1.2% vs 3.6%; p = 0.02), representing a 70% decrease in non-diabetics (p < 0.05) and 56.1% in diabetics (not significant). The observed overall incidence of acute postoperative dialysis was adequately predicted by the Cleveland Clinic Severity Score in the Control group (p = 0.6), but was lower than predicted in the Insulin group (1.2% vs 3%, p = 0.03).
Conclusions: In non-diabetic patients, tight perioperative blood glucose control is associated with a significant reduction in postoperative renal impairment and failure after cardiac surgery according to the RIFLE criteria. In non-diabetics, tight blood glucose control was associated with a decreased need for postoperative dialysis, as well as 30-day mortality, despite of a relatively short ICU stay.
Figures
References
-
- Ouattara A, Lecomte P, Le Manach Y, Landi M, Jacqueminet S, Platonov I, Bonnet N, Riou B, Coriat P. Poor intraoperative blood glucose control is associated with a worsened hospital outcome after cardiac surgery in diabetic patients. Anesthesiology. 2005;103:687–694. doi: 10.1097/00000542-200510000-00006. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
