

Lanthanum carbonate reduces phosphorus burden in patients with CKD stages 3 and 4: a randomized trial
- PMID: 19056618
- PMCID: PMC2615694
- DOI: 10.2215/CJN.02830608
Lanthanum carbonate reduces phosphorus burden in patients with CKD stages 3 and 4: a randomized trial
Abstract
Background and objectives: Lanthanum carbonate (FOSRENOL, Shire Pharmaceuticals) is an effective noncalcium, nonresin phosphate binder for the control of hyperphosphatemia in chronic kidney disease (CKD) stage 5 patients undergoing dialysis.
Design, setting, participants and measurements: A Phase 2, randomized, double-blind, placebo-controlled trial evaluating the efficacy and safety of lanthanum carbonate in CKD stage 3 and 4 patients. Of 281 patients screened, 121 were randomized (2:1) to lanthanum carbonate or placebo (80 versus 41). The modified intent-to-treat population included 90 patients (56 versus 34); 71 (43 versus 28) completed the study. After run-in, when any current phosphate binders were discontinued and dietary counseling reinforced, patients with serum phosphorus >4.6 mg/dl received lanthanum carbonate (titrated up to 3000 mg/d) or matching placebo for 8 wk.
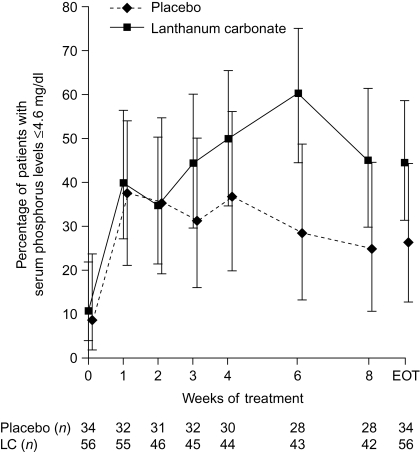
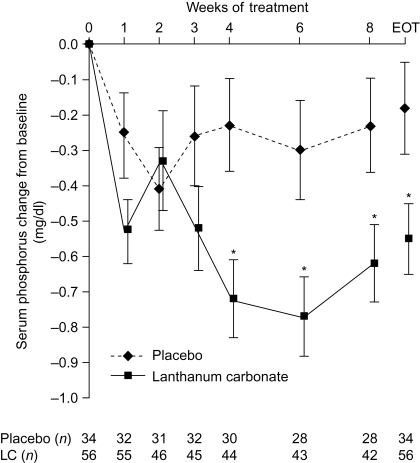
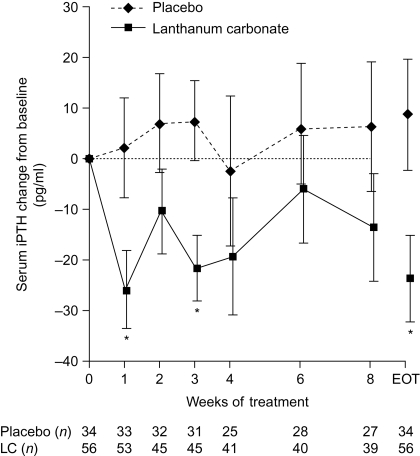
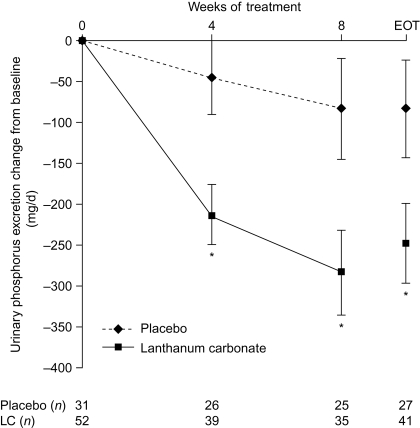
Results: At the end of treatment, 25 (44.6%) versus nine (26.5%) patients had serum phosphorus < or =4.6 mg/dl (difference 18.1%, P = 0.12) in the lanthanum carbonate and placebo groups, respectively. Statistically significant differences were observed between groups in change from baseline to end of treatment for serum phosphorus (P = 0.02), intact parathyroid hormone (P = 0.02), and urinary phosphorus excretion (P = 0.04). The safety profile and tolerability of lanthanum carbonate were similar to that of placebo.
Conclusions: Because <1% of phosphorus is in the extracellular fluid, serum measurements may not accurately reflect total body burden in patients with CKD stages 3 and 4. However, lanthanum carbonate is an effective phosphate binder in this patient population, with a safety profile and tolerability similar to that of placebo.
Trial registration: ClinicalTrials.gov NCT00234702.
Figures

References
-
- US Renal Data System. Atlas of End-Stage Renal Disease in the United States. National Institute of Diabetes and Digestive and Kidney Diseases, Bethesda, MD, 2000
-
- Tonelli M, Wiebe N, Culleton B, House A, Rabbat C, Fok M, McAlister F, Garg AX: Chronic kidney disease and mortality risk: A systematic review. J Am Soc Nephrol 17: 2034–2047, 2006 - PubMed
-
- Culleton BF, Larson MG, Wilson PW, Evans JC, Parfrey PS, Levy D: Cardiovascular disease and mortality in a community-based cohort with mild renal insufficiency. Kidney Int 56: 2214–2219, 1999 - PubMed
-
- Kestenbaum B, Sampson JN, Rudser KD, Patterson DJ, Seliger SL, Young B, Sherrard DJ, Andress DL: Serum phosphate levels and mortality risk among people with chronic kidney disease. J Am Soc Nephrol 16: 520–528, 2005 - PubMed
-
- Russo D, Palmiero G, De Blasio AP, Balletta MM, Andreucci VE: Coronary artery calcification in patients with CRF not undergoing dialysis. Am J Kidney Dis 44: 1024–1030, 2004 - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
