

Stepping responses of infants with myelomeningocele when supported on a motorized treadmill
- PMID: 19056853
- PMCID: PMC2614450
- DOI: 10.2522/ptj.20080120
Stepping responses of infants with myelomeningocele when supported on a motorized treadmill
Abstract
Background and purpose: Infants with myelomeningocele (MMC) have difficulty with, and show delays in, acquiring functional skills, such as walking. This study examined whether infants with MMC will respond to treadmill practice by producing stepping patterns or at least motor activity during the first year after birth. This study also compared the stepping trajectories of infants with MMC across age with those of infants with typical development (TD) to analyze the characteristics of the development of stepping patterns in infants with MMC early in life.
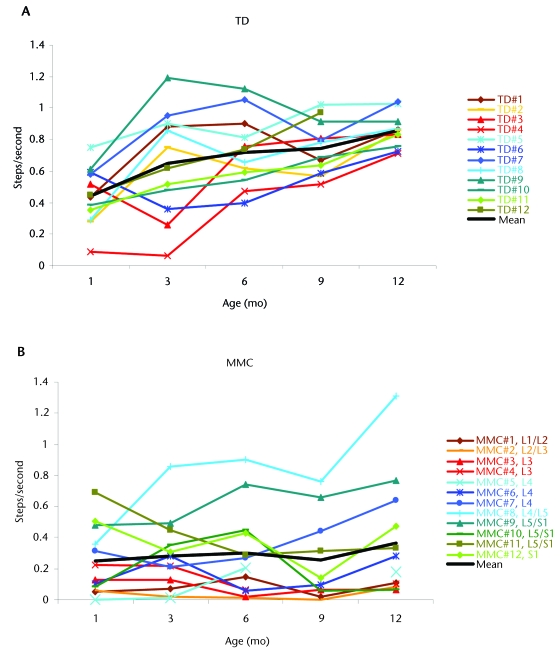
Participants: Twelve infants with MMC (lumbar and sacral lesions) and 12 infants with TD were the participants in this study.
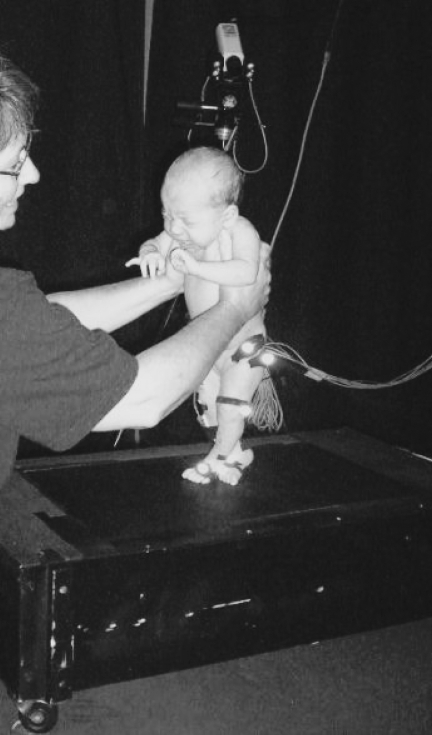
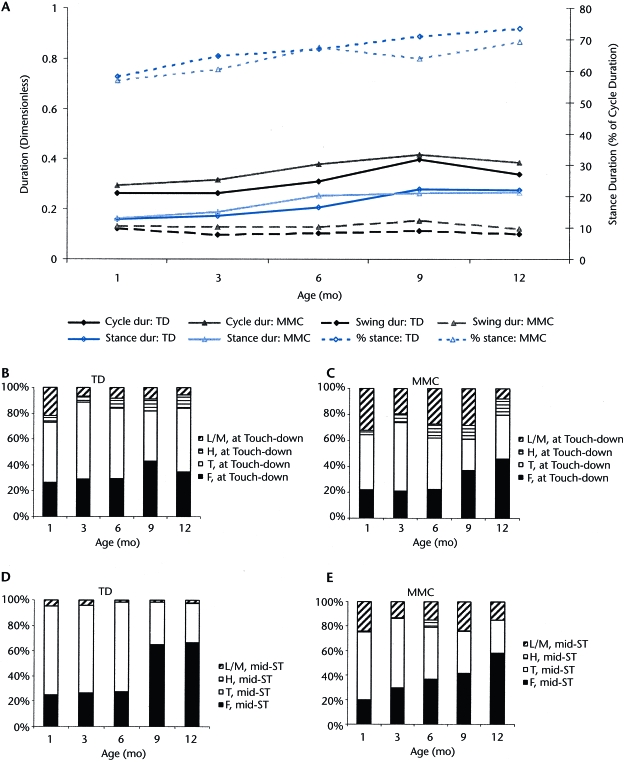
Methods: The infants were tested on a treadmill at ages 1, 3, 6, 9, and 12 months, with no treadmill practice between test sessions. Infants were supported on the treadmill for twelve 20-second trials. A digital camera and behavior coding were used to determine step rate, interlimb stepping patterns, step parameters, and motor activity level.
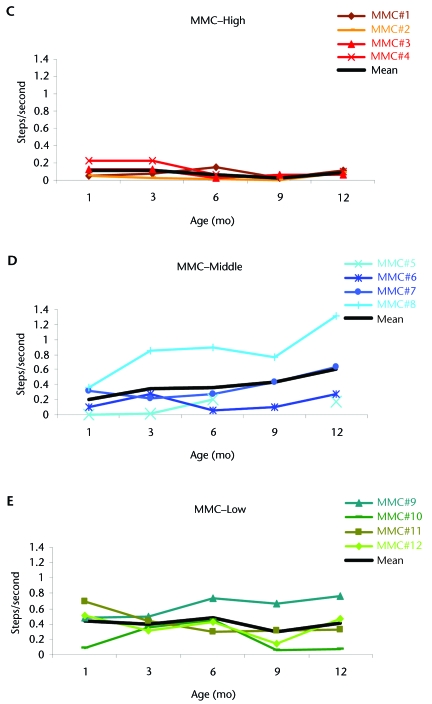
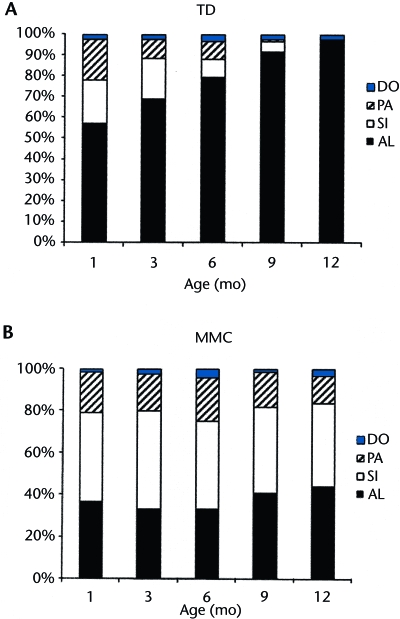
Results: Treadmill practice elicited steps in infants with MMC (14.4 steps/minute during the year) but less so than in infants with TD (40.8 steps/minute). Responsiveness was affected by lesion level but varied markedly among infants. Interlimb stepping was less readily alternating, but step parameters were similar to those produced by their peers with TD. Finally, holding infants with MMC on a moving treadmill resulted in greater motor activity (17% during the year) than holding infants on a nonmoving treadmill.
Discussion and conclusion: Infants with MMC responded to the treadmill by stepping (but less so than infants with TD) and showing increased motor activity, but they demonstrated a different developmental trajectory. Future studies are needed to explore the impact of enhancing sensory input during treadmill practice to optimize responses in infants with MMC.
Figures
References
-
- Spina Bifida Fact Sheet. Bethesda, MD: National Institute of Neurological Disorders and Stroke; 2007. NIH Publication No. 07–309.
-
- Cherian A, Seena S, Bullock RK, Antony AC. Incidence of neural tube defects in the least-developed area of India: a population-based study. Lancet. 2005;366:930–931. - PubMed
-
- Lary JM, Edmonds LD. Prevalence of spina bifida at birth—United States, 1983–1990: a comparison of two surveillance systems. MMWR CDC Surveill Summ. 1996;45:15–26. - PubMed
-
- International Clearinghouse for Birth Defects Monitoring Systems. World Atlas for Birth Defects/International Centre for Birth Defects of the International Clearinghouse for Birth Defects Monitoring Systems. 2nd ed. Geneva, Switzerland: World Health Organization; 2003.
-
- Duffy CM, Hill AE, Cosgrove AP, et al. Three dimensional analysis in spina bifida. J Pediatr Orthop. 1996;16:786–791. - PubMed
