

Weaning and extubation readiness in pediatric patients
- PMID: 19057432
- PMCID: PMC2849975
- DOI: 10.1097/PCC.0b013e318193724d
Weaning and extubation readiness in pediatric patients
Abstract
Objective: A systematic review of weaning and extubation for pediatric patients on mechanical ventilation.
Data selection: Pediatric and adult literature, English language.
Study selection: Invited review.
Data sources: Literature review using National Library of Medicine PubMed from January 1972 until April 2008, earlier cross-referenced article citations, the Cochrane Database of Systematic Reviews, and the Internet.
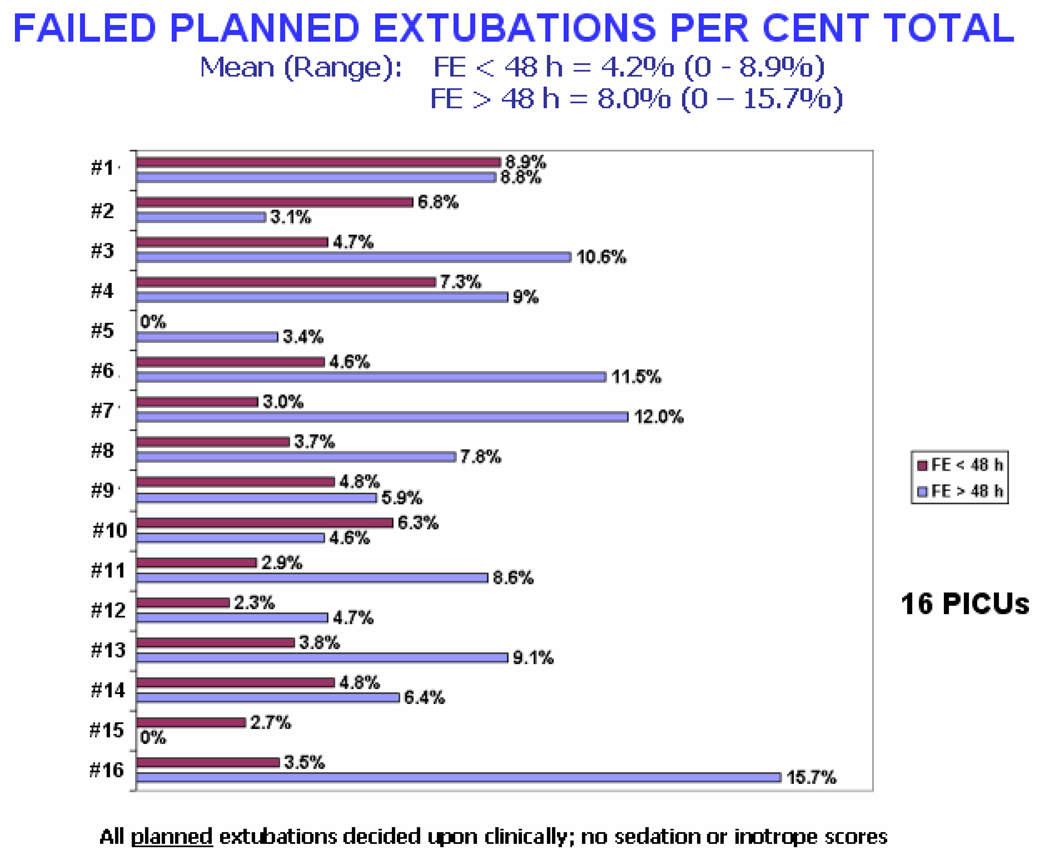
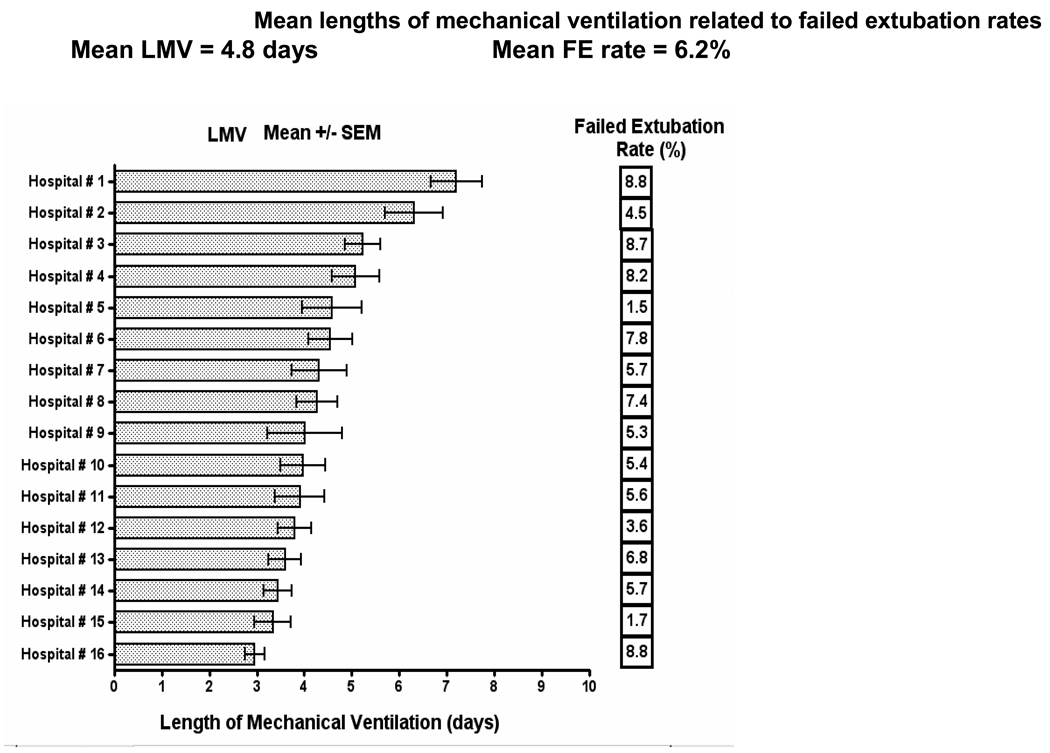
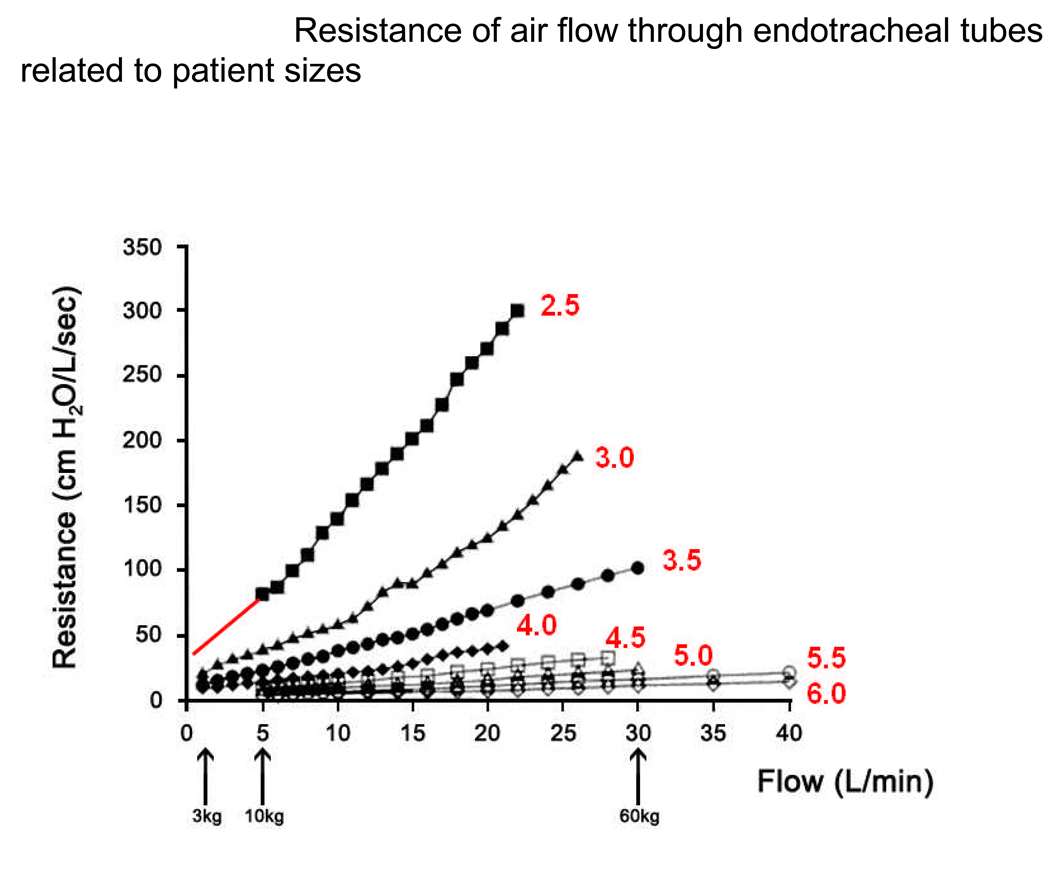
Conclusions: Despite the importance of minimizing time on mechanical ventilation, only limited guidance on weaning and extubation is available from the pediatric literature. A significant proportion of patients being evaluated for weaning are actually ready for extubation, suggesting that weaning is often not considered early enough in the course of ventilation. Indications for extubation are even less clear, although a trial of spontaneous breathing would seem a prerequisite. Several indices have been developed in an attempt to predict weaning and extubation success but the available literature would suggest they offer no improvement over clinical judgment. Extubation failure rates range from 2% to 20% and bear little relationship to the duration of mechanical ventilation. Upper airway obstruction is the single most common cause of extubation failure. A reliable method of assessing readiness for weaning and predicting extubation success is not evident from the pediatric literature.
Figures
Comment in
-
Do we know when to say "wean"?Pediatr Crit Care Med. 2009 Jan;10(1):126-7. doi: 10.1097/PCC.0b013e31819375fd. Pediatr Crit Care Med. 2009. PMID: 19131869 No abstract available.
References
-
- Khemani RG, Markovitz BP, Curley MAQ. Epidemiologic factors of mechanically ventilated PICU patients in the United States. Pediatr Crit Care Med. 2007;8:A39.
-
- Esteban A, Alia I, Gordo F, et al. The Spanish Lung Failure Collaborative Group. Extubation outcome after spontaneous breathing trials with T-tube or pressure support ventilation. Am J Respir Crit Care Med. 1997;156(2 Pt 1):459–465. - PubMed
-
- Farias JA, Retta A, Alia I, et al. A comparison of two methods to perform a breathing trial before extubation in pediatric intensive care patients. Intensive Care Med. 2001;27(10):1649–1654. - PubMed
-
- Epstein SK, Ciubotaru RL, Wong JB. Effect of failed extubation on the outcome of mechanical ventilation. Chest. 1997;112(1):186–192. - PubMed
Publication types
MeSH terms
Grants and funding
- U10HD049945/HD/NICHD NIH HHS/United States
- U01HD049934/HD/NICHD NIH HHS/United States
- U10 HD050012/HD/NICHD NIH HHS/United States
- U10 HD049945/HD/NICHD NIH HHS/United States
- U10HD049981/HD/NICHD NIH HHS/United States
- UG1 HD050096/HD/NICHD NIH HHS/United States
- U10 HD049981/HD/NICHD NIH HHS/United States
- U10 HD050096/HD/NICHD NIH HHS/United States
- U10 HD049983/HD/NICHD NIH HHS/United States
- RL1 HD107773/HD/NICHD NIH HHS/United States
- U10HD050096/HD/NICHD NIH HHS/United States
- U10HD049983/HD/NICHD NIH HHS/United States
- U10HD050012/HD/NICHD NIH HHS/United States
- U01 HD049934/HD/NICHD NIH HHS/United States
- U10HD500009/HD/NICHD NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
