

Imaging and transcatheter arterial embolization for traumatic splenic injuries: review of the literature
- PMID: 19057735
- PMCID: PMC2592580
Imaging and transcatheter arterial embolization for traumatic splenic injuries: review of the literature
Abstract
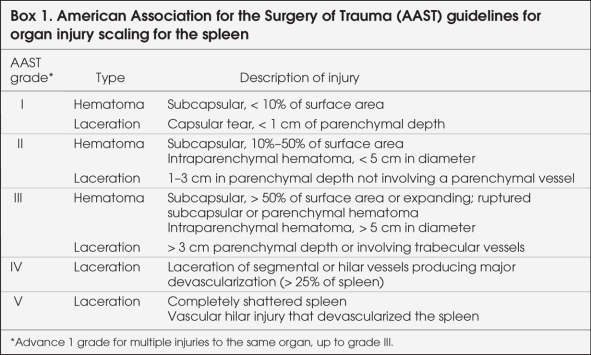
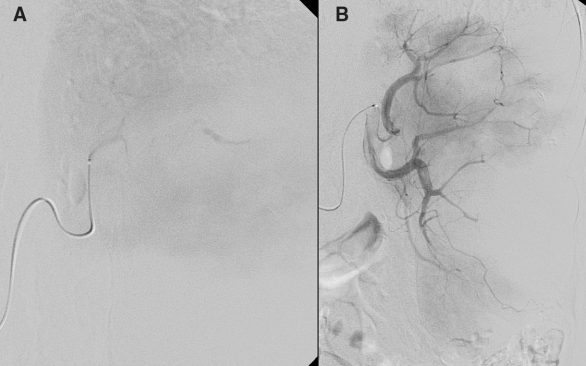
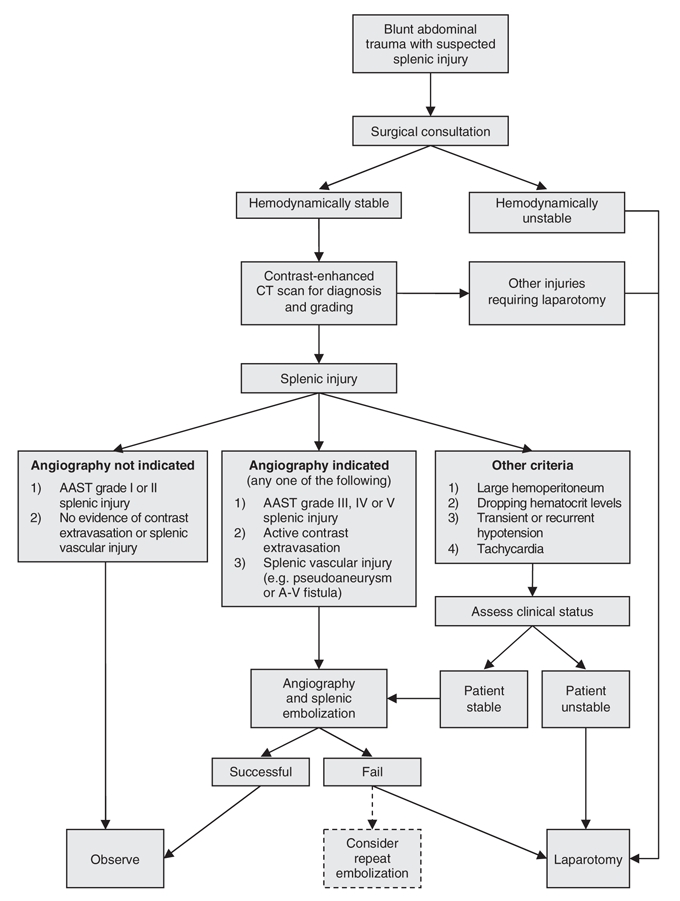
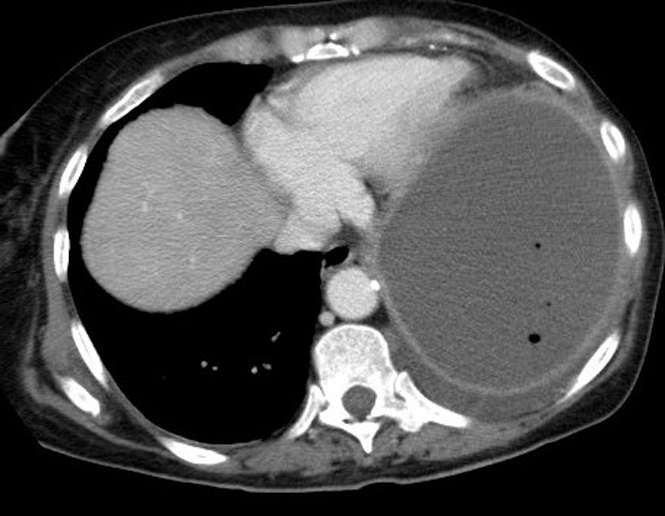
The spleen is the most commonly injured visceral organ in blunt abdominal trauma in both adults and children. Nonoperative management is the current standard of practice for patients who are hemodynamically stable. However, simple observation alone has been reported to have a failure rate as high as 34%; the rate is even higher among patients with high-grade splenic injuries (American Association for the Surgery of Trauma [AAST] grade III-V). Over the past decade, angiography with transcatheter splenic artery embolization, an alternative nonoperative treatment for splenic injuries, has increased splenic salvage rates to as high as 97%. With the help of splenic artery embolization, success rates of more than 80% have also been described for high-grade splenic injuries. We discuss the role of computed tomography and transcatheter splenic artery embolization in the diagnosis and treatment of blunt splenic trauma. We review technical considerations, indications, efficacy and complication rates. We also propose an algorithm to guide the use of angiography and splenic embolization in patients with traumatic splenic injury.
La rate est le viscère le plus souvent atteint dans les cas de traumatisme abdominal fermé tant chez l'adulte que chez l'enfant. La prise en charge non chirurgicale est la norme de pratique en vigueur pour les patients hémodynamiquement stables. On a toutefois signalé que l'observation simple, sans autre intervention, présente un taux d'échec pouvant atteindre 34 % et davantage chez les patients qui ont une lésion de la rate de grade élevé (American Association for the Surgery of Trauma [AAST] grades III–V). Au cours de la dernière décennie, l'angiographie avec embolisation de l'artère splénique par cathéter, solution de rechange au traitement non chirurgical des lésions de la rate, a porté jusqu'à 97 % les taux de préservation de la rate. On a aussi signalé que l'embolisation de l'artère splénique dans le cas de lésions de la rate de grade élevé produisait des taux de succès de plus de 80 %. Nous discutons du rôle de la tomodensitométrie et de l'embolisation de l'artère splénique par cathéter dans le diagnostic et le traitement du traumatisme fermé de la rate. Nous passons en revue les facteurs techniques, les indications, l'efficacité et les taux de complications. Nous proposons aussi un algorithme pour guider l'utilisation de l'angiographie et de l'embolisation de l'artère splénique chez les patients atteints de lésion traumatique de la rate.
Figures


References
-
- Robertson F, Leander P, Ekberg O. Radiology of the spleen. Eur Radiol 2001; 11: 80-95. - PubMed
-
- Schafermeyer R. Pediatric trauma. Emerg Med Clin North Am 1993;11:187-205. - PubMed
-
- Powell M, Courcoulas A, Gardner M, et al. Management of blunt splenic trauma: significant differences between adults and children. Surgery 1997;122: 654-60. - PubMed
-
- Moore EE, Cogbill TH, Jurkovich GJ, et al. Organ injury scaling: spleen and liver (1994 revision). J Trauma 1995;38:323-4. - PubMed
-
- Mirvis SE, Whitley NO, Gens DR. Blunt splenic trauma in adults: CT-based classification and correlation with prognosis and treatment. Radiology 1989;171:33-9. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous