

Surgical reduction of dysesthetic blebs
- PMID: 19064861
- PMCID: PMC2775801
- DOI: 10.1001/archophthalmol.2008.508
Surgical reduction of dysesthetic blebs
Abstract
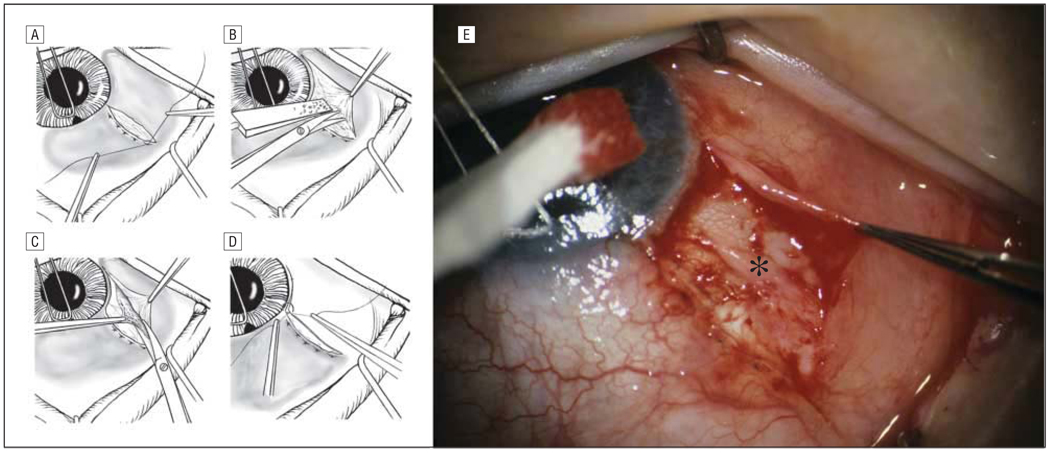
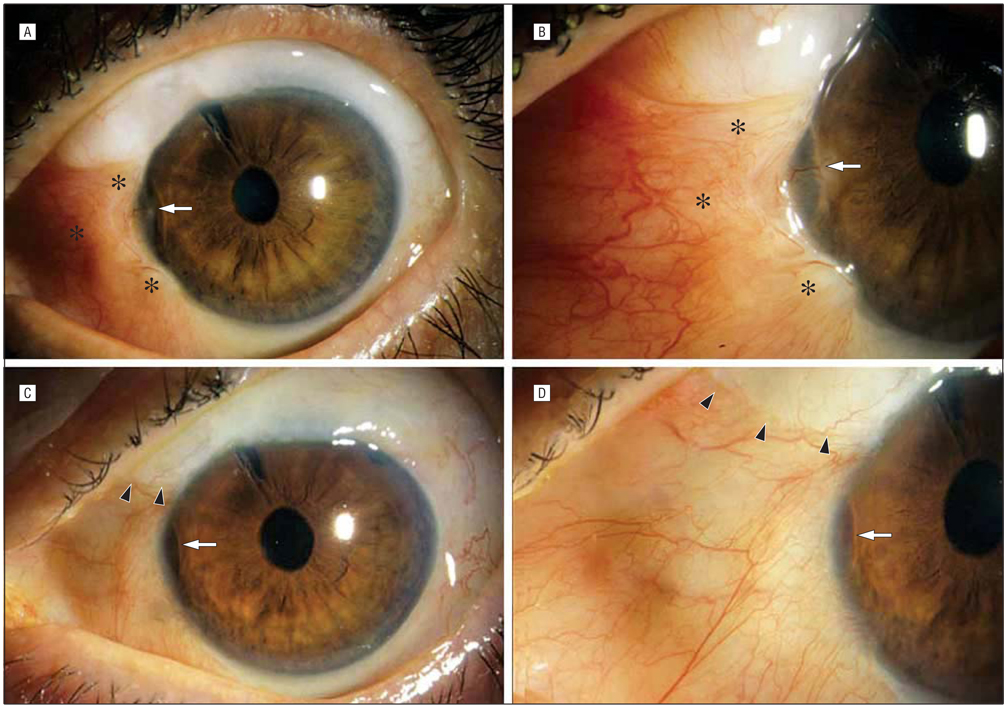
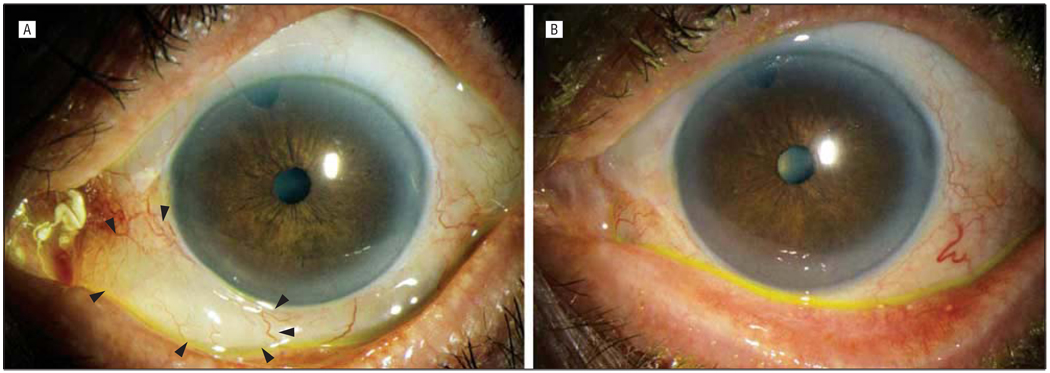
Dysesthetic blebs can complicate filtration surgery. Lubrication often reduces symptoms; however, some cases require surgical intervention. Limited conjunctivoplasty reduces the symptoms of dysesthetic blebs without sacrificing control of intraocular pressure (IOP). However, this may not sufficiently lower these blebs, particularly if the bleb is thick and dense. We describe a modified conjunctivoplasty technique that includes removal of subconjunctival scar tissue within the interpalpebral fissure and provide a 1-year follow-up of 13 eyes treated in this manner. All patients reported rapid, complete symptom resolution. The IOP was controlled in all 13 eyes following conjunctivoplasty; 3 required topical antiglaucoma therapy. Subconjunctival scar tissue may contribute to the formation of dysesthetic blebs owing to its thickness and by encouraging local dissection of aqueous humor. Our report demonstrates that removal of this tissue does not compromise IOP control when performed with conjunctivoplasty.
Figures
References
-
- Budenz DL, Hoffman K, Zacchei A. Glaucoma filtering bleb dysesthesia. Am J Ophthalmol. 2001;131(5):626–630. - PubMed
-
- Gehring JR, Ciccarelli EC. Trichloroacetic acid treatment of filtering blebs following cataract extraction. Am J Ophthalmol. 1972;74(4):622–624. - PubMed
-
- Wise JB. Treatment of chronic postfiltration hypotony by intrableb injection of autologous blood. Arch Ophthalmol. 1993;111(6):827–830. - PubMed
-
- Palmberg P. Late complications after glaucoma filtering surgery. In: Leader B, Calckwood J, editors. Proceedings of the 45th Annual Symposium of the New Orleans Academy of Ophthalmology; The Hague, the Netherlands. Kugler Publications; 1996.
