

Incidence of cardiovascular disease and cancer in advanced age: prospective cohort study
- PMID: 19066258
- PMCID: PMC2600919
- DOI: 10.1136/bmj.a2467
Incidence of cardiovascular disease and cancer in advanced age: prospective cohort study
Abstract
Objective: To investigate the influence of increasing age on the incidence and remaining lifetime risk of cardiovascular disease and cancer in a cohort of older men.
Design: Prospective cohort study.
Setting: United States.
Participants: 22,048 male doctors aged 40-84 who were free of major disease in 1982.
Main outcome measures: Incidence and remaining lifetime risk of major cardiovascular disease (myocardial infarction, stroke, and death from cardiovascular disease) and cancer.
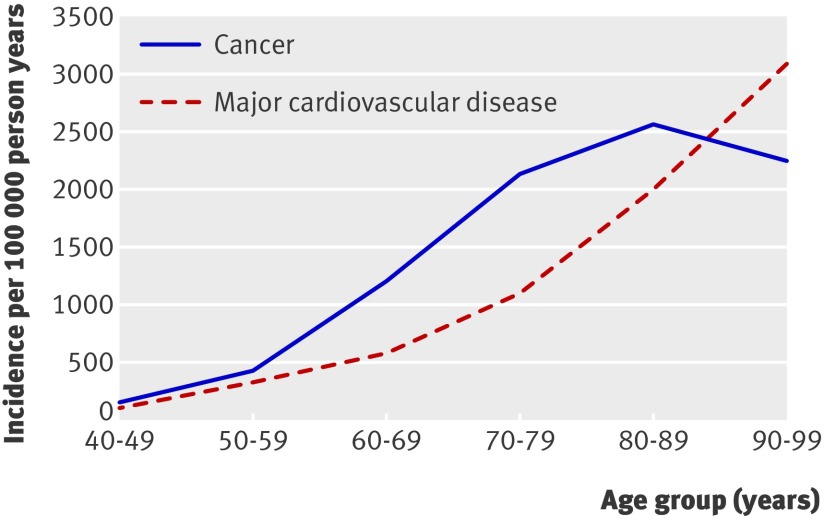
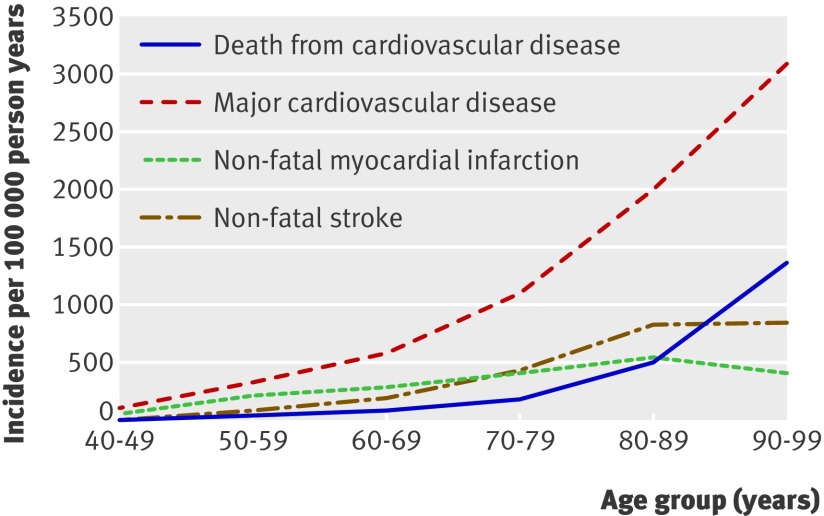
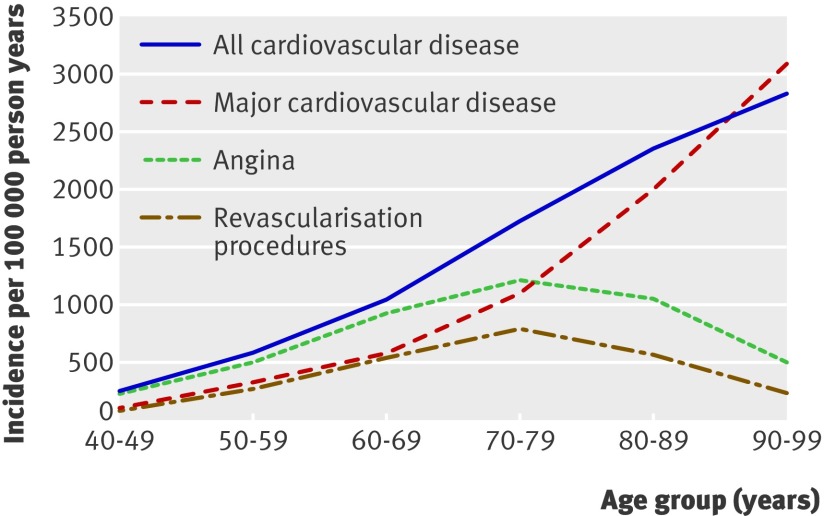
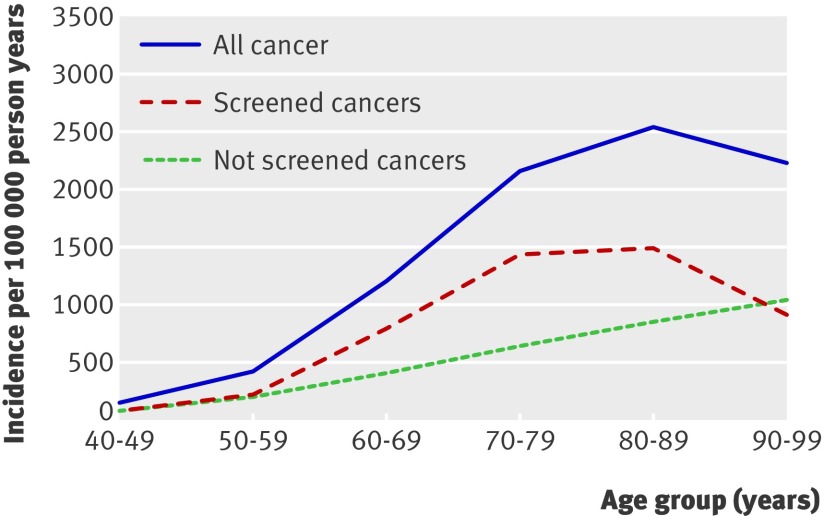
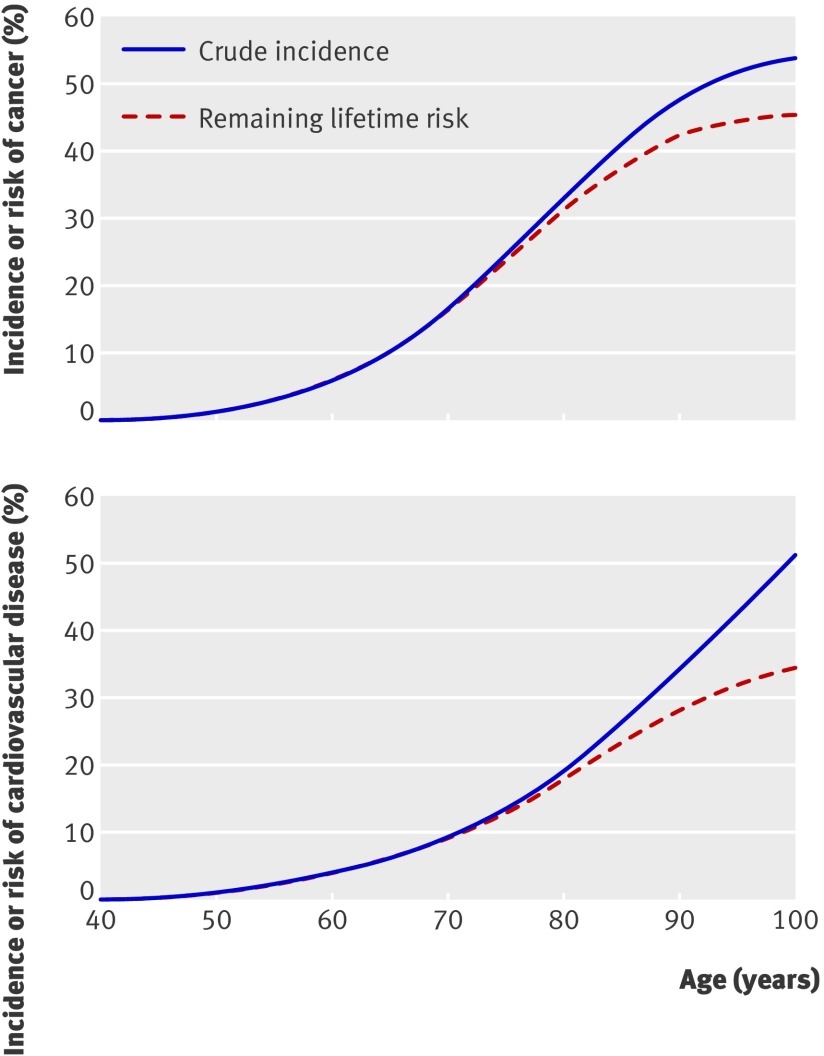
Results: 3252 major cardiovascular events and 5400 incident cancers were confirmed over 23 years of follow-up. The incidence of major cardiovascular disease continued to increase to age 100. Beginning at age 80, however, major cardiovascular disease was more likely to be diagnosed at death. The incidence of cancer peaked in those aged 80-89 and then declined. Cancers detected by screening accounted for most of the decline, whereas most cancers for which there was no screening continued to increase to age 100. Unadjusted cumulative incidence overestimated the risk of cardiovascular disease by 16% and cancer by 8.5%. The remaining lifetime risk of cancer at age 40 was 45.1% (95% confidence interval 43.8% to 46.3%) and at age 90 was 9.6% (7.2% to 11.9%). The remaining lifetime risk of major cardiovascular disease at age 40 was 34.8% (33.1% to 36.5%) and at age 90 was 16.7% (12.9% to 20.6%).
Conclusions: In this prospective cohort of men, the incidence of new cardiovascular disease continued to increase after age 80 but was most often diagnosed at death. The decrease in incidence of cancer late in life seemed largely due to a decline in cancers usually detected by screening. These findings suggest that people aged 80 and older have a substantial amount of undiagnosed disease. The remaining lifetime risk of both diseases approached a plateau in the 10th decade. This may be due to decreased detection of disease and reporting of symptoms and increased resistance to disease in those who survive to old age. Accurate estimates of disease risk in an aging population require adjustment for competing risks of mortality.
Conflict of interest statement
Competing interests: Although the authors believe they have no competing interests that could influence their decisions, work, or writing of the manuscript, they report a full disclosure for the past five years. LD received investigator initiated funding and support as principal investigator from the National Institutes of Health, the Alcoholic Beverage Medical Research Foundation, the Biomedical Research Institute at Brigham and Women’s Hospital, and the Huntington Disease Society of America. GL received investigator initiated research funding from the National Institutes of Health and received honorariums from Pfizer and Lilly Pharmaceutical for speaking engagements in 2003. JMG received investigator initiated research funding and support as principal investigator from the National Institutes of Health, BASF, DSM Pharmaceuticals, Wyeth Pharmaceuticals, McNeil Consumer Products, and Pliva; received honorariums from Bayer and Pfizer for speaking engagements; and is a consultant for Bayer, McNeil Consumer Products, Wyeth Pharmaceuticals, Merck, Nutraquest, and GlaxoSmithKline. TK received investigator initiated research funding as principal investigator or co-investigator from the National Institutes of Health, Bayer AG, McNeil Consumer & Specialty Pharmaceuticals, Merck, and Wyeth Consumer Healthcare; he is a consultant to i3 Drug Safety, and received honorariums from Organon for contributing to an expert panel and from Genzyme for providing educational lectures.
Figures
Comment in
-
Cardiovascular disease and cancer in very old age.BMJ. 2008 Dec 10;337:a2521. doi: 10.1136/bmj.a2521. BMJ. 2008. PMID: 19073659 No abstract available.
References
-
- World Health Organization. The top ten causes of death. WHO fact sheet. Geneva: WHO, 2007.
-
- Bray F, Moller B. Predicting the future burden of cancer. Nat Rev Cancer 2006;6:63-74. - PubMed
-
- Murray CJ, Lopez AD. Alternative projections of mortality and disability by cause 1990-2020: global burden of disease study. Lancet 1997;349:1498-504. - PubMed
-
- De Rijke JM, Schouten LJ, Hillen HF, Kiemeney LA, Coebergh JW, van den Brandt PA. Cancer in the very elderly Dutch population. Cancer 2000;89:1121-33. - PubMed
-
- Lloyd-Jones DM, Larson MG, Beiser A, Levy D. Lifetime risk of developing coronary heart disease. Lancet 1999;353:89-92. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources