

Delayed neural network degeneration after neonatal hypoxia-ischemia
- PMID: 19067347
- PMCID: PMC2605201
- DOI: 10.1002/ana.21517
Delayed neural network degeneration after neonatal hypoxia-ischemia
Abstract
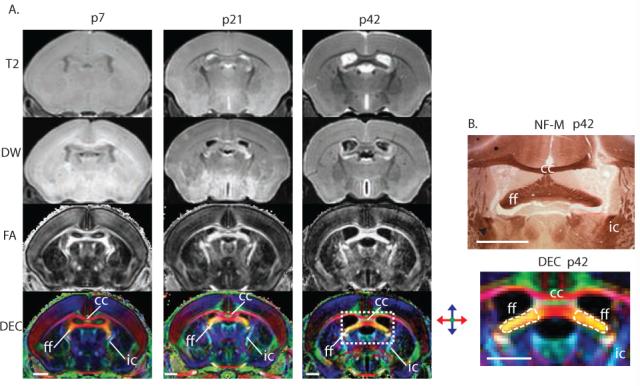
Objective: Clinical magnetic resonance studies show delayed and ongoing neurodegeneration after neonatal hypoxia-ischemia (HI), but the mechanisms and timing of this neurodegeneration remain unclear. We used ex vivo diffusion tensor imaging (DTI) and brain neuropathology to determine whether selective injury to white matter tracts occurs after neonatal HI in mice resulting in neural system-associated attrition in remote regions and at delayed times.
Methods: The Rice-Vannucci model (unilateral carotid ligation + 45 minutes of hypoxia FiO(2) = 0.08) was used to cause brain injury in postnatal day 7 (p7) C57BL6 mice, and ex vivo DTI and correlative neuropathology were performed at p8, p11, p15, p21, p28, and p42.
Results: DTI provides excellent contrast visualization of unmyelinated white matter in the immature mouse brain. Severe ipsilateral injury to the hippocampus is seen with both histopathology and diffusion-weighted magnetic resonance imaging 24 hours after injury. Injury to axons is evident 24 hours after HI in the hippocampal alveus. By p11 and continuing until p28, the ipsilateral fimbria fornix degenerates. At p15, there is injury and loss of axons entering the ipsilateral septal nucleus followed by ipsilateral septal atrophy. Volume loss in the hippocampus is rapid and severe, but is subacute and significantly slower in the ipsilateral septum. Neonatal HI also interrupts the normal developmental increase in fractional anisotropy in the ipsilateral fimbria but not in the contralateral fimbria from p8 to p42.
Interpretation: In neonatal brain, there is progressive systems-preferential injury after HI. DTI allows unparalleled visualization of this neural network-associated attrition so that it can be followed longitudinally in developing brain.
Figures





References
-
- Nelson KB, Grether JK. Causes of cerebral palsy. Curr Opin Pediatr. 1999;11:487–491. - PubMed
-
- Ferriero DM. Neonatal brain injury. N Engl J Med. 2004;351:1985–1995. - PubMed
-
- Hagberg H, Ichord R, Palmer C, et al. Animal models of developmental brain injury: relevance to human disease. A summary of the panel discussion from the Third Hershey Conference on Developmental Cerebral Blood Flow and Metabolism. Developmental neuroscience. 2002;24:364–366. - PubMed
-
- Folkerth RD. Neuropathologic substrate of cerebral palsy. J Child Neurol. 2005;20:940–949. - PubMed
-
- Rees S, Inder T. Fetal and neonatal origins of altered brain development. Early Hum Dev. 2005;81:753–761. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
