

The long-term effects of a peer-led sex education programme (RIPPLE): a cluster randomised trial in schools in England
- PMID: 19067478
- PMCID: PMC2586352
- DOI: 10.1371/journal.pmed.0050224
The long-term effects of a peer-led sex education programme (RIPPLE): a cluster randomised trial in schools in England
Abstract
Background: Peer-led sex education is widely believed to be an effective approach to reducing unsafe sex among young people, but reliable evidence from long-term studies is lacking. To assess the effectiveness of one form of school-based peer-led sex education in reducing unintended teenage pregnancy, we did a cluster (school) randomised trial with 7 y of follow-up.
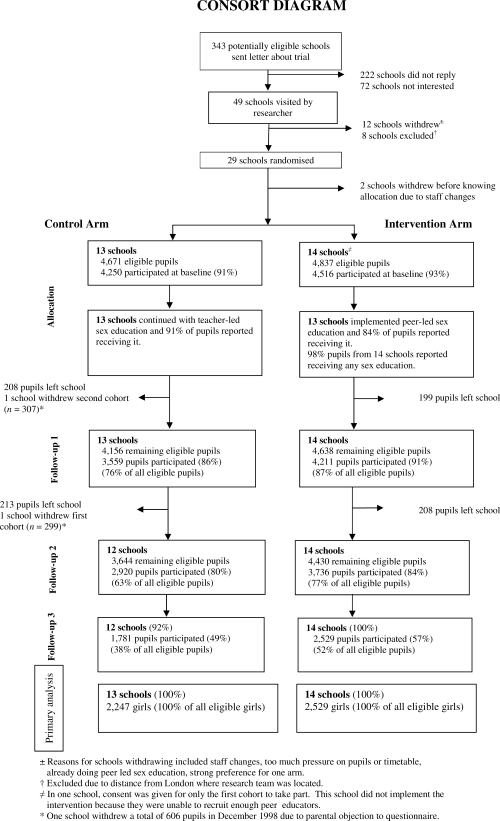
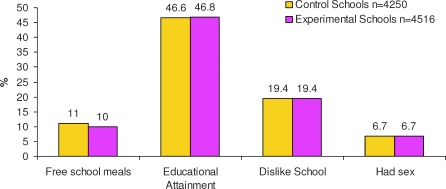
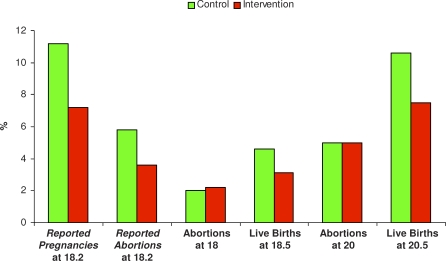
Methods and findings: Twenty-seven representative schools in England, with over 9,000 pupils aged 13-14 y at baseline, took part in the trial. Schools were randomised to either peer-led sex education (intervention) or to continue their usual teacher-led sex education (control). Peer educators, aged 16-17 y, were trained to deliver three 1-h classroom sessions of sex education to 13- to 14-y-old pupils from the same schools. The sessions used participatory learning methods designed to improve the younger pupils' skills in sexual communication and condom use and their knowledge about pregnancy, sexually transmitted infections (STIs), contraception, and local sexual health services. Main outcome measures were abortion and live births by age 20 y, determined by anonymised linkage of girls to routine (statutory) data. Assessment of these outcomes was blind to sex education allocation. The proportion of girls who had one or more abortions before age 20 y was the same in each arm (intervention, 5.0% [95% confidence interval (CI) 4.0%-6.3%]; control, 5.0% [95% CI 4.0%-6.4%]). The odds ratio (OR) adjusted for randomisation strata was 1.07 (95% CI 0.80-1.42, p = 0.64, intervention versus control). The proportion of girls with one or more live births by 20.5 y was 7.5% (95% CI 5.9%-9.6%) in the intervention arm and 10.6% (95% CI 6.8%-16.1%) in the control arm, adjusted OR 0.77 (0.51-1.15). Fewer girls in the peer-led arm self-reported a pregnancy by age 18 y (7.2% intervention versus 11.2% control, adjusted OR 0.62 [95% CI 0.42-0.91], weighted for non-response; response rate 61% intervention, 45% control). There were no significant differences for girls or boys in self-reported unprotected first sex, regretted or pressured sex, quality of current sexual relationship, diagnosed sexually transmitted diseases, or ability to identify local sexual health services.
Conclusion: Compared with conventional school sex education at age 13-14 y, this form of peer-led sex education was not associated with change in teenage abortions, but may have led to fewer teenage births and was popular with pupils. It merits consideration within broader teenage pregnancy prevention strategies.
Conflict of interest statement
Figures
References
-
- Independent Advisory Group on Sexual Health & HIV . Sex, drugs, alcohol and young people. A review of the impact of drugs and alcohol have on young people's sexual behaviour. London: Department of Health; 2007.
-
- The UK Collaborative Group for HIV and STI Surveillance. A complex picture: HIV and other STIs in the UK 2006. London: Health Protection Agency, Centre for Infections; 2006.
-
- Department of Health. Social Exclusion Unit. Teenage Pregnancy. London: Department of Health; 1999.
-
- Department of Education and Skills. Sex and relationship education guidance. 2003. Available: www.dfes.gov.uk. Report number: DFES 0116/2000. Accessed 28 October 2008.
-
- Sciacca JP. Student peer health education: a powerful yet inexpensive helping strategy. The Peer Facilitator Quarterly. 1987;5:4–6.
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
