

Modelling the impact of artemisinin combination therapy and long-acting treatments on malaria transmission intensity
- PMID: 19067479
- PMCID: PMC2586356
- DOI: 10.1371/journal.pmed.0050226
Modelling the impact of artemisinin combination therapy and long-acting treatments on malaria transmission intensity
Abstract
Background: Artemisinin derivatives used in recently introduced combination therapies (ACTs) for Plasmodium falciparum malaria significantly lower patient infectiousness and have the potential to reduce population-level transmission of the parasite. With the increased interest in malaria elimination, understanding the impact on transmission of ACT and other antimalarial drugs with different pharmacodynamics becomes a key issue. This study estimates the reduction in transmission that may be achieved by introducing different types of treatment for symptomatic P. falciparum malaria in endemic areas.
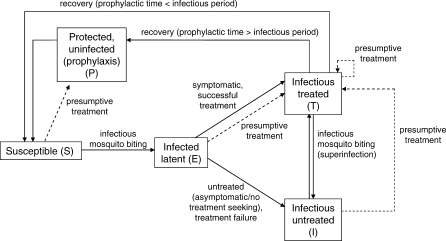
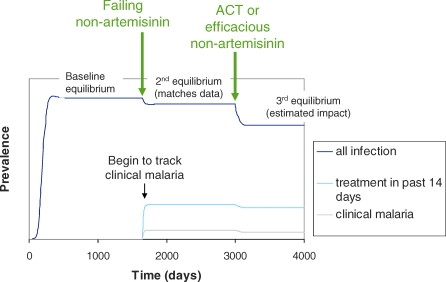
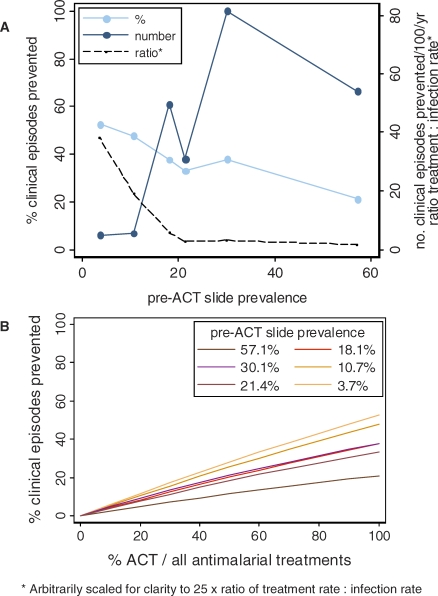
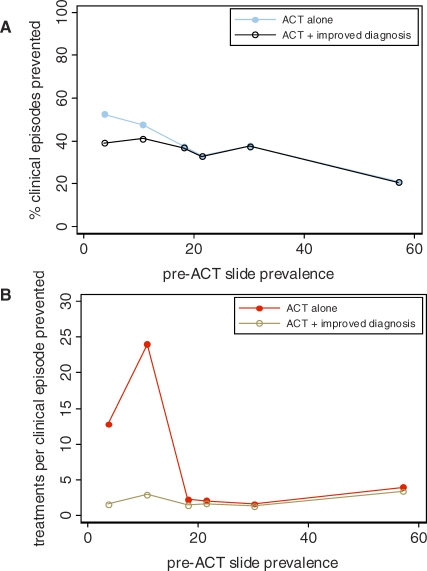
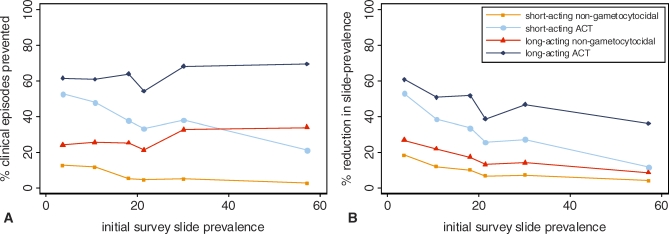
Methods and findings: We developed a mathematical model to predict the potential impact on transmission outcomes of introducing ACT as first-line treatment for uncomplicated malaria in six areas of varying transmission intensity in Tanzania. We also estimated the impact that could be achieved by antimalarials with different efficacy, prophylactic time, and gametocytocidal effects. Rates of treatment, asymptomatic infection, and symptomatic infection in the six study areas were estimated using the model together with data from a cross-sectional survey of 5,667 individuals conducted prior to policy change from sulfadoxine-pyrimethamine to ACT. The effects of ACT and other drug types on gametocytaemia and infectiousness to mosquitoes were independently estimated from clinical trial data. Predicted percentage reductions in prevalence of infection and incidence of clinical episodes achieved by ACT were highest in the areas with low initial transmission. A 53% reduction in prevalence of infection was seen if 100% of current treatment was switched to ACT in the area where baseline slide-prevalence of parasitaemia was lowest (3.7%), compared to an 11% reduction in the highest-transmission setting (baseline slide prevalence = 57.1%). Estimated percentage reductions in incidence of clinical episodes were similar. The absolute size of the public health impact, however, was greater in the highest-transmission area, with 54 clinical episodes per 100 persons per year averted compared to five per 100 persons per year in the lowest-transmission area. High coverage was important. Reducing presumptive treatment through improved diagnosis substantially reduced the number of treatment courses required per clinical episode averted in the lower-transmission settings although there was some loss of overall impact on transmission. An efficacious antimalarial regimen with no specific gametocytocidal properties but a long prophylactic time was estimated to be more effective at reducing transmission than a short-acting ACT in the highest-transmission setting.
Conclusions: Our results suggest that ACTs have the potential for transmission reductions approaching those achieved by insecticide-treated nets in lower-transmission settings. ACT partner drugs and nonartemisinin regimens with longer prophylactic times could result in a larger impact in higher-transmission settings, although their long term benefit must be evaluated in relation to the risk of development of parasite resistance.
Conflict of interest statement
Figures
References
-
- Bosman A, Mendis KN. A major transition in malaria treatment: the adoption and deployment of artemisinin-based combination therapies. Am J Trop Med Hyg. 2007;77:193–197. - PubMed
-
- Bjorkman A, Bhattarai A. Public health impact of drug resistant Plasmodium falciparum malaria. Acta Trop. 2005;94:163–169. - PubMed
-
- Bousema JT, Schneider P, Gouagna LC, Drakeley CJ, Tostmann A, et al. Moderate effect of artemisinin-based combination therapy on transmission of Plasmodium falciparum . J Infect Dis. 2006;193:1151–1159. - PubMed
-
- Drakeley CJ, Jawara M, Targett GA, Walraven G, Obisike U, et al. Addition of artesunate to chloroquine for treatment of Plasmodium falciparum malaria in Gambian children causes a significant but short-lived reduction in infectiousness for mosquitoes. Trop Med Int Health. 2004;9:53–61. - PubMed
-
- Sutherland CJ, Ord R, Dunyo S, Jawara M, Drakeley CJ, et al. Reduction of malaria transmission to anopheles mosquitoes with a six-dose regimen of co-artemether. PLoS Med. 2005;2:e92. doi: 10.1371/journal.pmed.0020092. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
