

The two stage model of preeclampsia: variations on the theme
- PMID: 19070896
- PMCID: PMC2680383
- DOI: 10.1016/j.placenta.2008.11.009
The two stage model of preeclampsia: variations on the theme
Abstract
The Two Stage Model of preeclampsia proposes that a poorly perfused placenta (Stage 1) produces factor(s) leading to the clinical manifestations of preeclampsia (Stage 2). Stage 1 is not sufficient to cause the maternal syndrome but interacts with maternal constitutional factors (genetic, behavioral or environmental) to result in Stage 2. Recent information indicates the necessity for modifications of this model. It is apparent that changes relevant to preeclampsia and other implantation disorders can be detected in the first trimester, long before the failed vascular remodeling necessary to reduce placental perfusion is completed. In addition, although the factor(s) released from the placenta has usually been considered a toxin, we suggest that what is released may also be an appropriate signal from the fetal/placental unit to overcome reduced nutrient availability that cannot be tolerated by some women who develop preeclampsia. Further, it is evident that linkage is not likely to be one factor but several, different for different women. Also although the initial model limited the role of maternal constitutional factors to the genesis of Stage 2, this does not appear to be the case. It is evident that the factors increasing risk for preeclampsia are also associated with abnormal implantation. These several modifications have important implications. An earlier origin for Stage 1, which appears to be recognizable by altered concentrations of placental products, could allow earlier intervention. The possibility of a fetal placental factor increasing nutrient availability could provide novel therapeutic options. Different linkages and preeclampsia subtypes could direct specific preventive treatments for different women while the role of maternal constitutional factors to affect placentation provides targets for prepregnancy therapy. The modified Two Stage Model provides a useful guide towards investigating pathophysiology and guiding therapy.
Figures



 ) or the maternal constitution (
) or the maternal constitution ( ) to result in the maternal pathophysiological changes of preeclampsia can vary. It can be primarily fetal/placental (A), equally maternal constitutional and fetal/placental (B) or primarily maternal (C). It is a reasonable extension that some women with exquisite sensitivity to fetal/placental function could respond to the normal physiological changes of pregnancy (D).
) to result in the maternal pathophysiological changes of preeclampsia can vary. It can be primarily fetal/placental (A), equally maternal constitutional and fetal/placental (B) or primarily maternal (C). It is a reasonable extension that some women with exquisite sensitivity to fetal/placental function could respond to the normal physiological changes of pregnancy (D).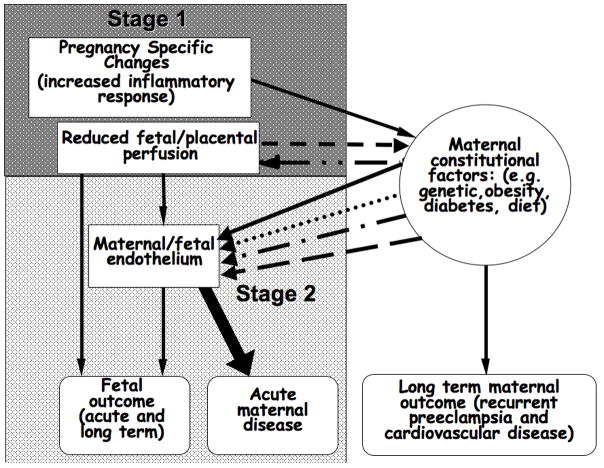
 ) modify maternal physiology, which cannot be tolerated by women resulting in preeclampsia. The same maternal constitutional changes that interact with abnormal placentation can also stimulate abnormal placentation (
) modify maternal physiology, which cannot be tolerated by women resulting in preeclampsia. The same maternal constitutional changes that interact with abnormal placentation can also stimulate abnormal placentation ( ). Also the linkage between Stage 1 and Stage 2 is likely secondary to many factors (several 305 arrows compared to one in the original model).
). Also the linkage between Stage 1 and Stage 2 is likely secondary to many factors (several 305 arrows compared to one in the original model).References
-
- Roberts J. Pre-eclampsia a two-stage disorder: What is the linkage? Are there directed fetal/placental signals? In: FL, MB, editors. Pre-eclampsia: Etiology and clinical practice. New York: Cambridge University Press; 2007. pp. 183–194.
-
- Khong TY, De Wolf F, Robertson WB, Brosens I. Inadequate maternal vascular response to placentation in pregnancies complicated by pre-eclampsia and by small-for-gestational age infants. British Journal of Obstetrics and Gynaecology. 1986;93:1049–1059. - PubMed
-
- Arias F, Rodriquez L, Rayne SC, Kraus FT. Maternal placental vasculopathy and infection: Two distinct subgroups among patients with preterm labor and preterm ruptured membranes. Am J Obstet Gynecol. 1993;168:585–91. - PubMed
-
- Schipper EJI, Bolte AC, Schalkwijk CG, Van Geijn HP, Dekker GA. Tnf-receptor levels in preeclampsia - results of a longitudinal study in high-risk women. Journal Of Maternal-Fetal & Neonatal Medicine. 2005;18:283–287. - PubMed
-
- Maynard SE, Venkatesha S, Thadhani R, Karumanchi SA. Soluble fms-like tyrosine kinase 1 and endothelial dysfunction in the pathogenesis of preeclampsia. Pediatric Research. 2005;57:1R–7R. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
