

doi: 10.1371/journal.pmed.0050241.
What is the future for global case management guidelines for common childhood diseases?
Affiliations
- PMID: 19071957
- PMCID: PMC2596856
- DOI: 10.1371/journal.pmed.0050241
Item in Clipboard
What is the future for global case management guidelines for common childhood diseases?
PLoS Med.
.
Abstract
Mike English and J. Anthony G. Scott propose a framework for national surveillance, monitoring, and research that could help inform guideline development in low-income settings.
Conflict of interest statement
Figures
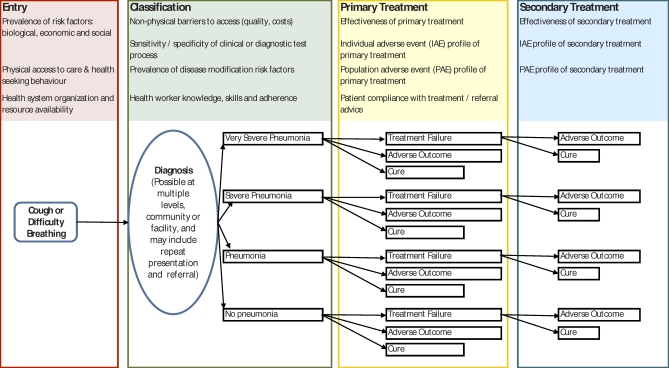
Contextual factors are likely to operate from the stage at which they first appear on the left-hand side of the figure right through to the far right of the figure. The list shown is illustrative and not exhaustive. Consider the possible effects of introducing Haemophilus influenzae type b and pneumococcal conjugate vaccines. As the relative prevalence of bacterial pneumonia declines, the positive predictive value of any imperfect clinical or diagnostic test used to assign children to antibiotic treatment will also fall, and so the population benefits of antibiotic therapy will also decline. This will increase the proportion of unnecessary treatments and enhance the importance of adverse effects at both the individual and population levels. Population adverse effects, for example the development of resistance, are likely to reflect total antibiotic use and can be included as additional probabilities associated with each treatment episode. For clarity these are not shown in the illustration but see [11] for an example. The effect of our current lack of basic data may be illustrated when we try to estimate the value of new treatments in a new setting. In the last ten years, most emerging evidence has come from comparative efficacy trials of primary treatments for pneumonia. However, while we now have data on the relative reduction in risk of treatment failure or mortality attributable to a new therapy, we cannot estimate absolute risk reduction at a specific country level because data on the risk of treatment failure or death associated with the “old” treatment in this setting are missing. Consider also recent calls from paediatricians in areas with a high prevalence of HIV for changes in the guidelines on treating hospitalised infants with severe pneumonia. If we know baseline risks, the incremental effectiveness of any newly proposed treatment, and the prevalence of HIV, we can estimate the aggregate outcomes of changing treatment for a given population. Additionally, the net benefits of such a change could be compared with alternative interventions elsewhere in the decision tree, such as changing the antibiotic used for outpatient treatment of pneumonia.
References
-
- Darmstadt G, Bhutta Z, Cousens S, Adam T, Walker N, et al. Evidence-based, cost-effective interventions: How many newborn babies can we save. Lancet. 2005;365:977–988. - PubMed
-
- Jones G, Steketee RW, Black RE, Bhutta ZA, Morris SS, et al. How many child deaths can we prevent this year. Lancet. 2003;362:65–71. - PubMed
-
- Oxman AD, Lavis JN, Fretheim A. Use of evidence in WHO recommendations. Lancet. 2007;369:1883–1869. - PubMed
-
- Bhattarai A, Ali AS, Kachur SP, Mårtensson A, Abbas AK, et al. Impact of artemisinin-based combination therapy and insecticide-treated nets on malaria burden in Zanzibar. PLoS Med. 2007;4:e309. doi: 10.1371/journal.pmed.0040309. - DOI - PMC - PubMed
