

Intracranial electroencephalography seizure onset patterns and surgical outcomes in nonlesional extratemporal epilepsy
- PMID: 19072306
- PMCID: PMC2841508
- DOI: 10.3171/2008.8.JNS17643
Intracranial electroencephalography seizure onset patterns and surgical outcomes in nonlesional extratemporal epilepsy
Abstract
Object: Patients with normal MR imaging (nonlesional) findings and medically refractory extratemporal epilepsy make up a disproportionate number of nonexcellent outcomes after epilepsy surgery. In this paper, the authors investigated the usefulness of intracranial electroencephalography (iEEG) in the identification of surgical candidates.
Methods: Between 1992 and 2002, 51 consecutive patients with normal MR imaging findings and extratemporal epilepsy underwent intracranial electrode monitoring. The implantation of intracranial electrodes was determined by seizure semiology, interictal and ictal scalp EEG, SPECT, and in some patients PET studies. The demographics of patients at the time of surgery, lobar localization of electrode implantation, duration of follow-up, and Engel outcome score were abstracted from the Mayo Rochester Epilepsy Surgery Database. A blinded independent review of the iEEG records was conducted for this study.
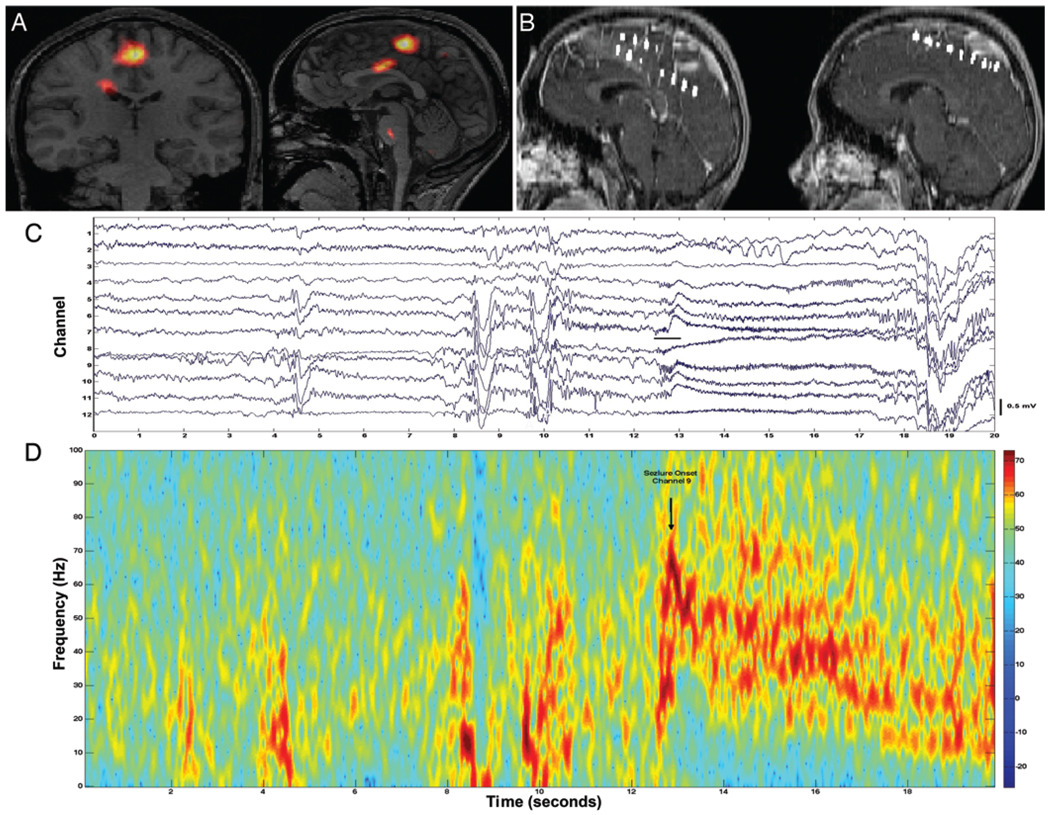
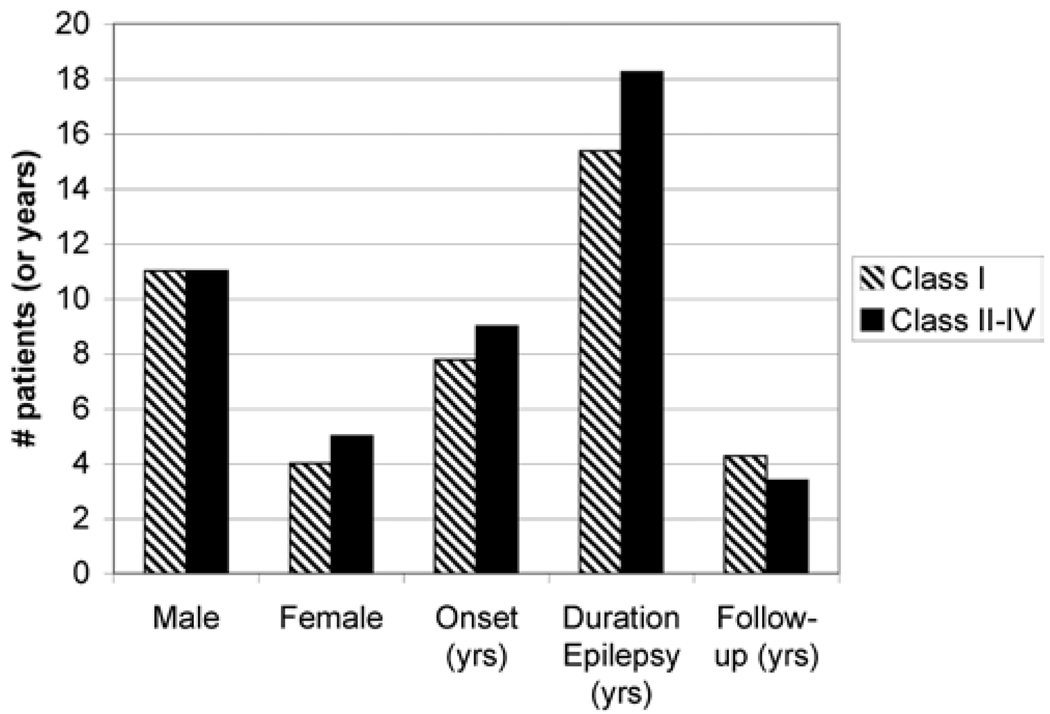
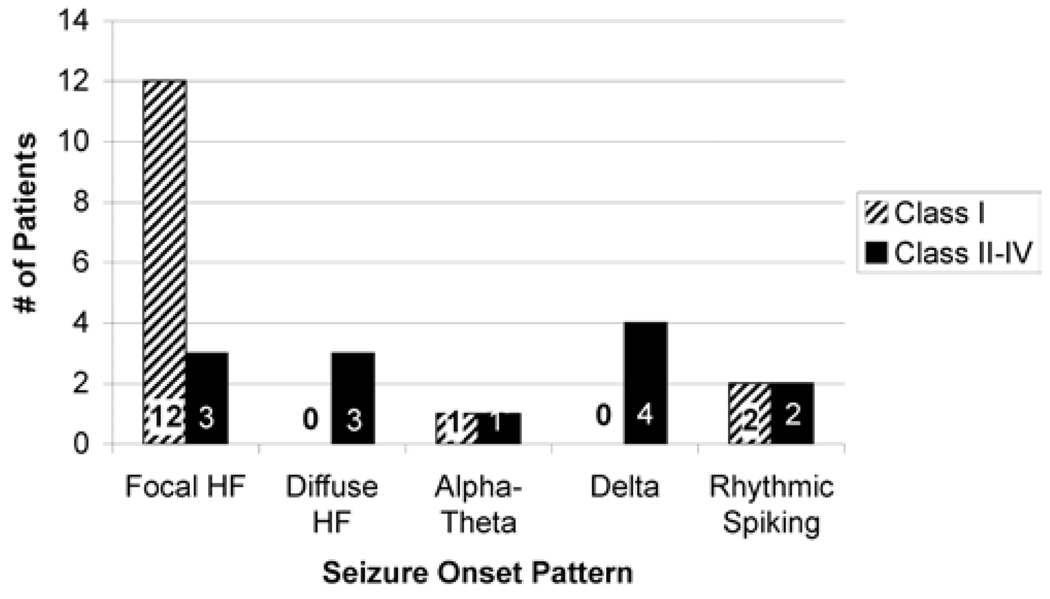
Results: Thirty-one (61%) of the 51 patients who underwent iEEG ultimately underwent resection for their epilepsy. For 28 (90.3%) of the 31 patients who had epilepsy surgery, adequate information regarding follow-up (> 1 year), seizure frequency, and iEEG recordings was available. Twenty-six (92.9%) of 28 patients had frontal lobe resections, and 2 had parietal lobe resections. The most common iEEG pattern at seizure onset in the surgically treated group was a focal high-frequency discharge (in 15 [53.6%] of 28 patients). Ten (35.7%) of the 28 surgically treated patients were seizure free. Fourteen (50%) had Engel Class I outcomes, and overall, 17 (60.7%) had significant improvement (Engel Class I and IIAB with > or =80% seizure reduction). Focal high-frequency oscillation at seizure onset was associated with Engel Class I surgical outcome (12 [85.7%] of 14 patients, p = 0.02), and it was uncommon in the nonexcellent outcome group (3 [21.4%] of 14 patients).
Conclusions: A focal high-frequency oscillation (> 20 Hz) at seizure onset on iEEG may identify patients with nonlesional extratemporal epilepsy who are likely to have an Engel Class I outcome after epilepsy surgery. The prospect of excellent outcome in nonlesional extratemporal lobe epilepsy prior to intracranial monitoring is poor (14 [27.5%] of 51 patients). However, iEEG can further stratify patients and help identify those with a greater likelihood of Engel Class I outcome after surgery.
Conflict of interest statement
The authors report no conflict of interest concerning the materials or methods used in this study or the findings specified in this paper.
Figures
References
-
- Akiyama T, Otsubo H, Ochi A, Galicia EZ, Weiss SK, Donner EJ, et al. Topographic movie of ictal high-frequency oscillations on the brain surface using subdural EEG in neocortical epilepsy. Epilepsia. 2006;47:1953–1957. - PubMed
-
- Akiyama T, Otsubo H, Ochi A, Ishiguro T, Kadokura G, Ramachandrannair R, et al. Focal cortical high-frequency oscillations trigger epileptic spasms: confirmation by digital video subdural EEG. Clin Neurophysiol. 2005;116:2819–2825. - PubMed
-
- Alarcon G, Binnie CD, Elwes RD, Polkey CE. Power spectrum and intracranial EEG patterns at seizure onset in partial epilepsy. Electroencephalogr Clin Neurophysiol. 1995;94:326–337. - PubMed
-
- Allen PJ, Fish DR, Smith SJ. Very high-frequency rhythmic activity during SEEG suppression in frontal lobe epilepsy. Electroencephalogr Clin Neurophysiol. 1992;82:155–159. - PubMed
-
- Bragin A, Engel J, Jr, Wilson CL, Fried I, Buzsaki G. High-frequency oscillations in human brain. Hippocampus. 1999;9:137–142. - PubMed
