

Where the O2 goes to: preservation of human fetal oxygen delivery and consumption at high altitude
- PMID: 19074967
- PMCID: PMC2670090
- DOI: 10.1113/jphysiol.2008.163634
Where the O2 goes to: preservation of human fetal oxygen delivery and consumption at high altitude
Abstract
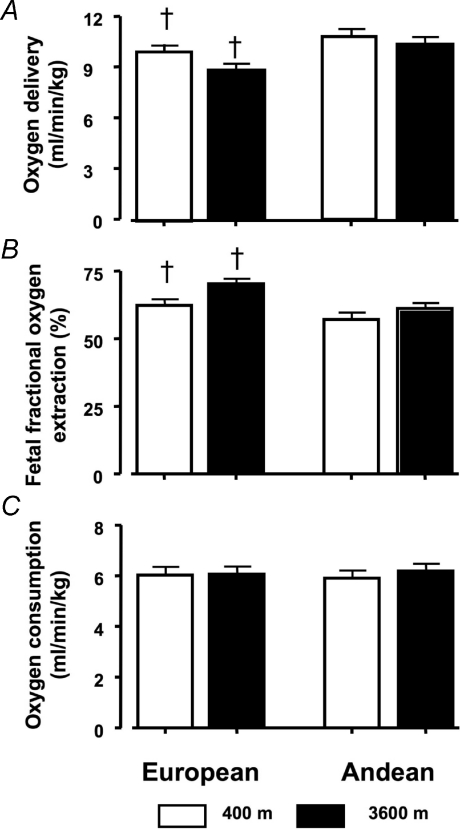
Fetal growth is decreased at high altitude (> 2700 m). We hypothesized that variation in fetal O(2) delivery might account for both the altitude effect and the relative preservation of fetal growth in multigenerational natives to high altitude. Participants were 168 women of European or Andean ancestry living at 3600 m or 400 m. Ancestry was genetically confirmed. Umbilical vein blood flow was measured using ultrasound and Doppler. Cord blood samples permitted calculation of fetal O(2) delivery and consumption. Andean fetuses had greater blood flow and oxygen delivery than Europeans and weighed more at birth, regardless of altitude (+208 g, P < 0.0001). Fetal blood flow was decreased at 3600 m (P < 0.0001); the decrement was similar in both ancestry groups. Altitude-associated decrease in birth weight was greater in Europeans (-417 g) than Andeans (-228 g, P < 0.005). Birth weight at 3600 m was > 200 g lower for Europeans at any given level of blood flow or O(2) delivery. Fetal haemoglobin concentration was increased, decreased, and the fetal / curve was left-shifted at 3600 m. Fetuses receiving less O(2) extracted more (r(2) = 0.35, P < 0.0001). These adaptations resulted in similar fetal O(2) delivery and consumption across all four groups. Increased umbilical venous O(2) delivery correlated with increased fetal O(2) consumption per kg weight (r(2) = 0.50, P < 0.0001). Blood flow (r(2) = 0.16, P < 0.001) and O(2) delivery (r(2) = 0.17, P < 0.001) correlated with birth weight at 3600 m, but not at 400 m (r(2) = 0.04, and 0.03, respectively). We concluded that the most pronounced difference at high altitude is reduced fetal blood flow, but fetal haematological adaptation and fetal capacity to increase O(2) extraction indicates that deficit in fetal oxygen delivery is unlikely to be causally associated with the altitude- and ancestry-related differences in fetal growth.
Figures


 and
and  determined by the blood gas analyses was plotted for each of the four groups using a third order polynomial (best fit regression). The low altitude curves overlap for Europeans (□) and Andeans (○). High altitude left-shifts the
determined by the blood gas analyses was plotted for each of the four groups using a third order polynomial (best fit regression). The low altitude curves overlap for Europeans (□) and Andeans (○). High altitude left-shifts the  /
/ curve (P < 0.05), with Andean fetuses (•, continuous line) showing a progressively greater leftward shift with increasing
curve (P < 0.05), with Andean fetuses (•, continuous line) showing a progressively greater leftward shift with increasing  when compared with the Europeans (▪, dashed–dotted line). This results in differences at which the blood is 50% saturated (indicated by the line at 50% on the y axis). The P50 for
when compared with the Europeans (▪, dashed–dotted line). This results in differences at which the blood is 50% saturated (indicated by the line at 50% on the y axis). The P50 for  is equivalent at 400 m (28.4 versus 28.5 for European (dotted line) and Andean (dashed line), respectively). In contrast the blood is half-saturated with oxygen at 25.8 mmHg at 3600 m in Europeans, and 23.4 mmHg at 3600 m in Andean, P < 0.05). The Andean fetuses at 3600 m thus maintain saturation at higher levels for a given
is equivalent at 400 m (28.4 versus 28.5 for European (dotted line) and Andean (dashed line), respectively). In contrast the blood is half-saturated with oxygen at 25.8 mmHg at 3600 m in Europeans, and 23.4 mmHg at 3600 m in Andean, P < 0.05). The Andean fetuses at 3600 m thus maintain saturation at higher levels for a given  when compared with Europeans. (400 m European y=–92.8 + 8.64x– (–0.16x2) + 0.001x3, r2= 0.94, P < 0.0001; 400 m Andean y=–16.4 + 1.09x+ 0.81x2– 0.001x3, r2= 0.97, P < 0.0001; 3600 m European y=–122.4 + 13.33x–0.32x2+ 0.003x3, r2= 0.90, P < 0.0001; 3600 m Andean y=–7.0 – 0.98x+ 0.24x2– 0.004x3, r2= 0.97, P < 0.0001.) B, the maternal curves relating
when compared with Europeans. (400 m European y=–92.8 + 8.64x– (–0.16x2) + 0.001x3, r2= 0.94, P < 0.0001; 400 m Andean y=–16.4 + 1.09x+ 0.81x2– 0.001x3, r2= 0.97, P < 0.0001; 3600 m European y=–122.4 + 13.33x–0.32x2+ 0.003x3, r2= 0.90, P < 0.0001; 3600 m Andean y=–7.0 – 0.98x+ 0.24x2– 0.004x3, r2= 0.97, P < 0.0001.) B, the maternal curves relating  to
to  are also left-shifted at high altitude, but without any apparent difference due to ethnicity at low or high altitude. The line symbols are the same as in A. (400 m European y=–9.6 + 2.94x– 0.81x2– 0.001x3, r2= 0.97, P < 0.0001; 3600 m European y=–122.4 + 13.13x– 0.32x2+ 0.003x3, r2= 0.91, P < 0.0001; 400 m Andean y=–15.7 + 1.02x+ 0.08x2– 0.001x3, r2= 0.97, P < 0.0001; 3600 m Andean y=–1.9 – 1.59x+ 0.27x2– 0.005x3, r2= 0.98, P < 0.0001.) C shows the correlation between maternal
are also left-shifted at high altitude, but without any apparent difference due to ethnicity at low or high altitude. The line symbols are the same as in A. (400 m European y=–9.6 + 2.94x– 0.81x2– 0.001x3, r2= 0.97, P < 0.0001; 3600 m European y=–122.4 + 13.13x– 0.32x2+ 0.003x3, r2= 0.91, P < 0.0001; 400 m Andean y=–15.7 + 1.02x+ 0.08x2– 0.001x3, r2= 0.97, P < 0.0001; 3600 m Andean y=–1.9 – 1.59x+ 0.27x2– 0.005x3, r2= 0.98, P < 0.0001.) C shows the correlation between maternal  and fetal
and fetal  at the two altitude combined. For any given value of maternal
at the two altitude combined. For any given value of maternal  , the Andean fetus has a lower
, the Andean fetus has a lower  than the European fetus. (y= 34.1 + 0.33x, r2= 0.06, P < 0.05 European; y= 30.4 + 0.46x, r2= 0.12, P < 0.005.)
than the European fetus. (y= 34.1 + 0.33x, r2= 0.06, P < 0.05 European; y= 30.4 + 0.46x, r2= 0.12, P < 0.005.)

 , such that those fetuses with the greatest O2 extraction have the lowest arterial
, such that those fetuses with the greatest O2 extraction have the lowest arterial  (r2= 0.64, P < 0.0001 all subjects). (400 m Europeans y= 34.6 – 0.29x, r2= 0.71, P < 0.0001; 3600 m Europeans y= 42.3 – 0.38x, r2= 0.69, P < 0.0001; 400 m Andean y= 29.6 + 0.20x, r2= 0.31, P < 0.0005; 3600 m Andean y= 32.0 – 0.26x, r2= 0.75, P < 0.0001.) The slope of the relationship is virtually identical between altitudes (centre inset right, P= 0.98), and did not differ between ancestry groups (P= 0.26).
(r2= 0.64, P < 0.0001 all subjects). (400 m Europeans y= 34.6 – 0.29x, r2= 0.71, P < 0.0001; 3600 m Europeans y= 42.3 – 0.38x, r2= 0.69, P < 0.0001; 400 m Andean y= 29.6 + 0.20x, r2= 0.31, P < 0.0005; 3600 m Andean y= 32.0 – 0.26x, r2= 0.75, P < 0.0001.) The slope of the relationship is virtually identical between altitudes (centre inset right, P= 0.98), and did not differ between ancestry groups (P= 0.26).
References
-
- Acharya G, Wilsgaard T, Berntsen GKR, Maltau JM, Kiserud T. Doppler-derived umbilical artery absolute velocities and their relationship to fetoplacental volume blood flow: a longitudinal study. Ultrasound Obstet Gynecol. 2005;25:444–453. - PubMed
-
- Alonso JG, Okai T, Longo LD, Gilbert RD. Cardiac function during long-term hypoxemia in fetal sheep. Am J Physiol Heart Circ Physiol. 1989;257:H581–H589. - PubMed
-
- Backe SK, Lyons G. Oxygen and elective caesarean section. Br J Anaesth. 2002;88:4–5. - PubMed
-
- Ballew C, Haas JD. Hematologic evidence of fetal hypoxia among newborn infants at high altitude in Bolivia. Am J Obstet Gynecol. 1986;155:166–169. - PubMed
-
- Barbera A, Galan HL, Ferrazzi E, Rigano S, Jozwik M, Battaglia FC, Pardi G. Relationship of umbilical vein blood flow to growth parameters in the human fetus. Am J Obstet Gynecol. 1999;181:174–179. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical