

Safety and efficacy of rasburicase (SR29142) in a Japanese phase II study
- PMID: 19076979
- PMCID: PMC11159938
- DOI: 10.1111/j.1349-7006.2008.01047.x
Safety and efficacy of rasburicase (SR29142) in a Japanese phase II study
Abstract
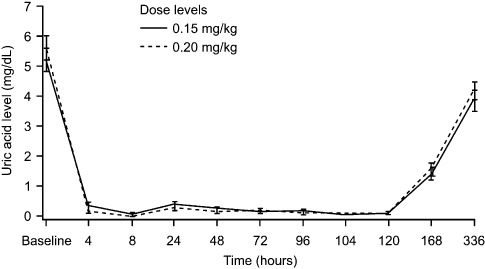
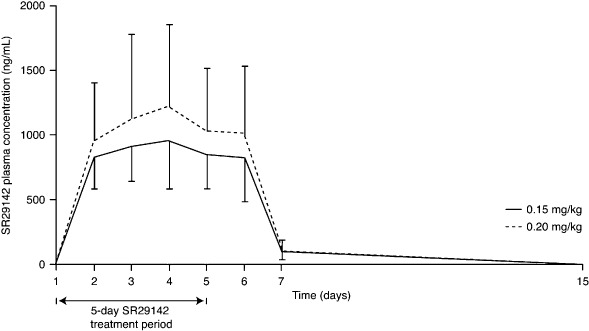
The purpose of this study was to investigate the safety profile of SR29142 when administered as a single agent both prior to chemotherapy and during treatment, and to compare the efficacy of SR29142 administered at two dose levels in adult Japanese patients with leukemia or lymphoma. During this open-label, multicenter, phase II study, patients received SR29142 for 5 days, administered at either 0.15 or 0.20 mg/kg per day. Chemotherapy was started 4–24 h after the first infusion of SR29142. The primary end-point was overall response rate, defined as the normalization of plasma uric acid to 7.5 mg/dL or less, from 48 h after the first infusion to 24 h after the last infusion of SR29142. SR29142-related adverse events including hypersensitivity (allergic) reactions were assessed. Overall, 50 patients received SR29142 at either 0.15 mg/kg per day (n = 25) or 0.20 mg/kg per day (n = 25) followed by chemotherapy. The overall response rate was 100.0% (95% confidence interval, 86.3–100.0%) with 0.15 mg/kg and 96.0% (95% confidence interval, 79.6–99.9%) with 0.20 mg/kg. Both dose levels of SR29142 were equally effective at reducing plasma uric acid levels. In six patients, seven drug-related adverse events of grade 1/2 occurred before chemotherapy. SR29142-related, hypersensitivity-associated reactions occurred in three patients, and rash, anorexia, application site pain and pyrexia occurred in one patient each; only five patients (10%) showed anti-SR29142 antibodies by day 29. In conclusion, SR29142 is effective at reducing plasma uric acid levels with a tolerable safety profile as a single agent both prior to chemotherapy and during treatment.
Trial registration: ClinicalTrials.gov NCT00631579.
Figures
References
-
- Cairo MS, Bishop M. Tumor lysis syndrome: new therapeutic strategies and classification. Br J Haematol 2004; 127: 3–11. - PubMed
-
- Del Toro G, Moris E, Cairo MS. Tumor lysis syndrome: pathophysiology, definition, and alternative treatment approaches. Clin Adv Hematol Oncol 2005; 3: 54–61. - PubMed
-
- Cheson BD, Frame JN, Vena D, Quashu N, Sorensen JM. Tumor lysis syndrome: an uncommon complication of fludarabine therapy of chronic lymphocytic leukemia. J Clin Oncol 1998; 16: 2313–20. - PubMed
-
- Annemans L, Moeremans K, Lamotte M et al . Incidence, medical resource utilisation and costs of hyperuricemia and tumour lysis syndrome in patients with acute leukaemia and non‐Hodgkin's lymphoma in four European countries. Leuk Lymphoma 2003; 44: 77–83. - PubMed
-
- Hagemeister F, Huen A. The status of allopurinol in the management of tumor lysis syndrome: a clinical review. Cancer J 2005; 11 (Suppl. 1): S1–S10. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
