

Use of pharmacokinetic/ pharmacodynamic modelling for starting dose selection in first-in-human trials of high-risk biologics
- PMID: 19076987
- PMCID: PMC2670372
- DOI: 10.1111/j.1365-2125.2008.03297.x
Use of pharmacokinetic/ pharmacodynamic modelling for starting dose selection in first-in-human trials of high-risk biologics
Abstract
What is already known about this subject: Recent regulatory guidance has highlighted the importance of using pharmacokinetic-pharmacodynamic (PK-PD) modelling in the selection of starting doses in first-in-human trials of high-risk biologics. However, limited examples exist in literature illustrating this procedure.
What this study adds: An interpretation of the recommended dose-selection methodology and the minimum anticipated biological effect level (MABEL) principle, contained in the updated European Medicines Agency guidance on risk-mitigation strategies for first-in-human studies, is presented. Some literature and simulation-based examples of the application of PK-PD modelling principles to starting dose selection using in vitro and in vivo data under the MABEL paradigm are highlighted, along with the advantages and limitations of this approach.
Aims: To illustrate the use of pharmacokinetic-pharmacodynamic (PK-PD) models to select rational starting doses in clinical trials within the minimum anticipated biological effect level (MABEL) principle using literature data and through simulations.
Methods: The new European Medicines Agency guidance on starting dose selection of high-risk biologics was analysed considering the basic pharmacological properties and preclinical testing limitations of many biologics. The MABEL approach to dose selection was illustrated through simulations and through literature-reported examples on the selection of starting doses for biologics such as antibodies based on in vitro biomarker data, in vivo PK and PK-PD data.
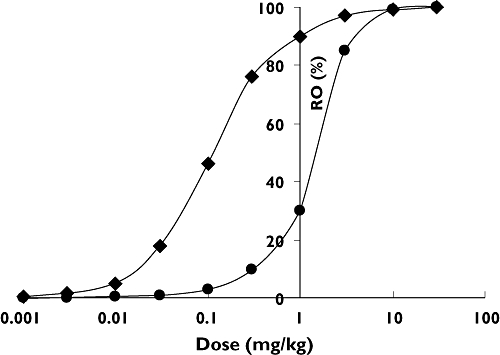
Results: Literature reports indicating the use of preclinical pharmacological and toxicological data to select successfully safe starting doses in line with the MABEL principle are summarized. PK-PD model-based simulations of receptor occupancy for an anti-IgE antibody system indicate that the relative abundance of IgE in animal models and patients and the turnover rate of the IgE-antibody complex relative to the off-rate of the antibody from IgE are important determinants of in vivo receptor occupancy.
Conclusions: Mechanistic PK-PD models are capable of integrating preclinical in vitro and in vivo data to select starting doses rationally in first-in-human trials. Biological drug-receptor interaction dynamics is complex and multiple factors affect the dose-receptor occupancy relationship. Thus, these factors should be taken into account when selecting starting doses.
Figures



References
-
- Duff G. Expert Scientific Group on Phase One Clinical Trials: Final Report. London: Department of Health, UK; 2006.
-
- FDA. Guidance for Industry: Estimating the Maximum Safe Starting Dose in Initial Clinical Trials for Therapeutics in Adult Healthy Volunteers. Rockville MD: FDA; 2005.
-
- Reigner BG, Blesch KS. Estimating the starting dose for entry into humans: principles and practice. Eur J Clin Pharmacol. 2002;57:835–45. - PubMed
-
- Vaidya AB, Vaidya RA. Initial human trials with an investigational new drug (phase 1 and 2): planning and management. J Postgrad Med. 1981;27:197–213. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
