

Association between administered oxygen, arterial partial oxygen pressure and mortality in mechanically ventilated intensive care unit patients
- PMID: 19077208
- PMCID: PMC2646321
- DOI: 10.1186/cc7150
Association between administered oxygen, arterial partial oxygen pressure and mortality in mechanically ventilated intensive care unit patients
Abstract
Introduction: The aim of this study was to investigate whether in-hospital mortality was associated with the administered fraction of oxygen in inspired air (FiO2) and achieved arterial partial pressure of oxygen (PaO2).
Methods: This was a retrospective, observational study on data from the first 24 h after admission from 36,307 consecutive patients admitted to 50 Dutch intensive care units (ICUs) and treated with mechanical ventilation. Oxygenation data from all admission days were analysed in a subset of 3,322 patients in 5 ICUs.
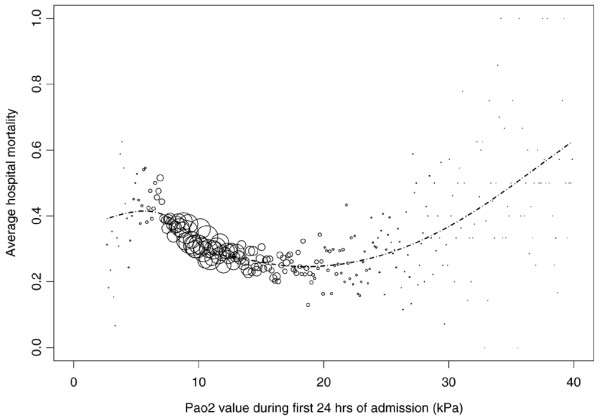
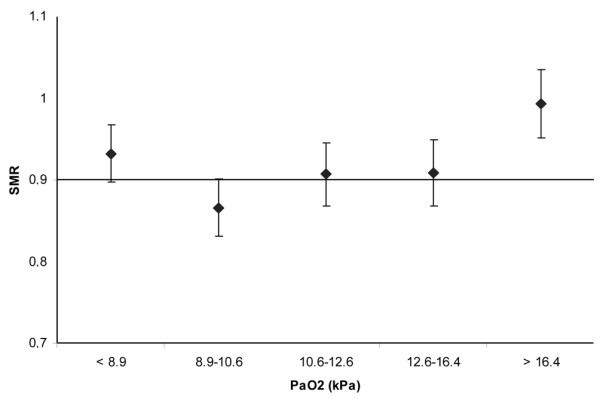
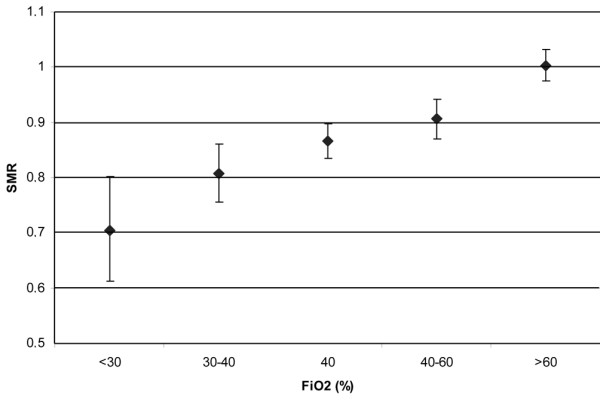
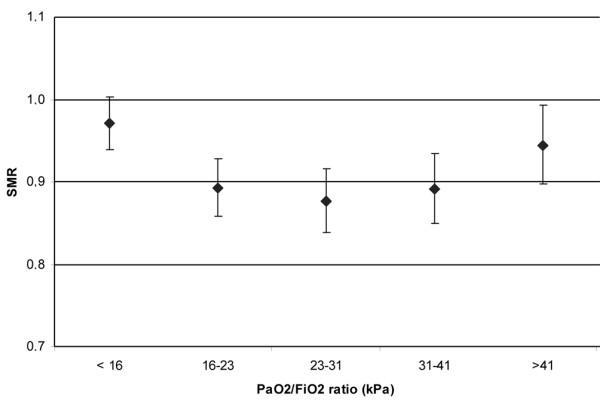
Results: Mean PaO2 and FiO2 in the first 24 h after ICU admission were 13.2 kPa (standard deviation (SD) 6.5) and 50% (SD 20%) respectively. Mean PaO2 and FiO2 from all admission days were 12.4 kPa (SD 5.5) and 53% (SD 18). Focusing on oxygenation in the first 24 h of admission, in-hospital mortality was shown to be linearly related to FiO2 value and had a U-shaped relationship with PaO2 (both lower and higher PaO2 values were associated with a higher mortality), independent of each other and of Simplified Acute Physiology Score (SAPS) II, age, admission type, reduced Glasgow Coma Scale (GCS) score, and individual ICU. Focusing on the entire ICU stay, in-hospital mortality was independently associated with mean FiO2 during ICU stay and with the lower two quintiles of mean PaO2 value during ICU stay.
Conclusions: Actually achieved PaO2 values in ICU patients in The Netherlands are higher than generally recommended in the literature. High FiO2, and both low PaO2 and high PaO2 in the first 24 h after admission are independently associated with in-hospital mortality in ICU patients. Future research should study whether this association is causal or merely a reflection of differences in severity of illness insufficiently corrected for in the multivariate analysis.
Figures
References
-
- Amato MB, Barbas CS, Medeiros DM, Magaldi RB, Schettino GP, Lorenzi-Filho G, Kairalla RA, Deheinzelin D, Munoz C, Oliveira R, Takagaki TY, Carvalho CR. Effect of a protective-ventilation strategy on mortality in the acute respiratory distress syndrome. N Engl J Med. 1998;338:347–354. doi: 10.1056/NEJM199802053380602. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
