

Long-term outcomes five years after selective dorsal rhizotomy
- PMID: 19077294
- PMCID: PMC2633339
- DOI: 10.1186/1471-2431-8-54
Long-term outcomes five years after selective dorsal rhizotomy
Abstract
Background: Selective dorsal rhizotomy (SDR) is a well accepted neurosurgical procedure performed for the relief of spasticity interfering with motor function in children with spastic cerebral palsy (CP). The goal is to improve function, but long-term outcome studies are rare. The aims of this study were to evaluate long-term functional outcomes, safety and side effects during five postoperative years in all children with diplegia undergoing SDR combined with physiotherapy.
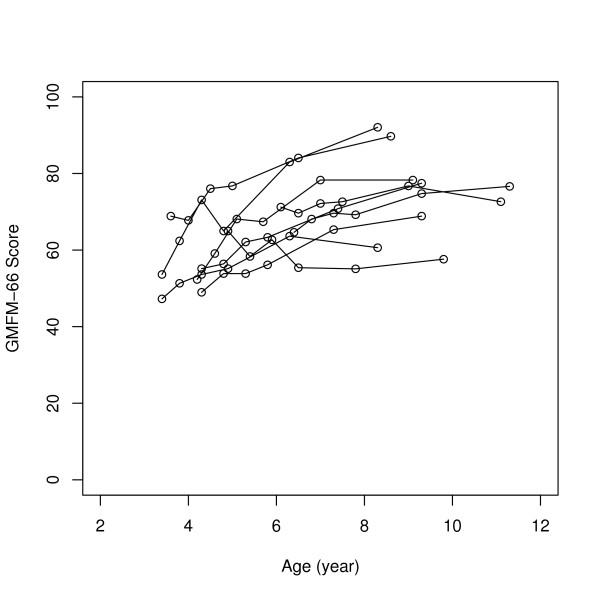
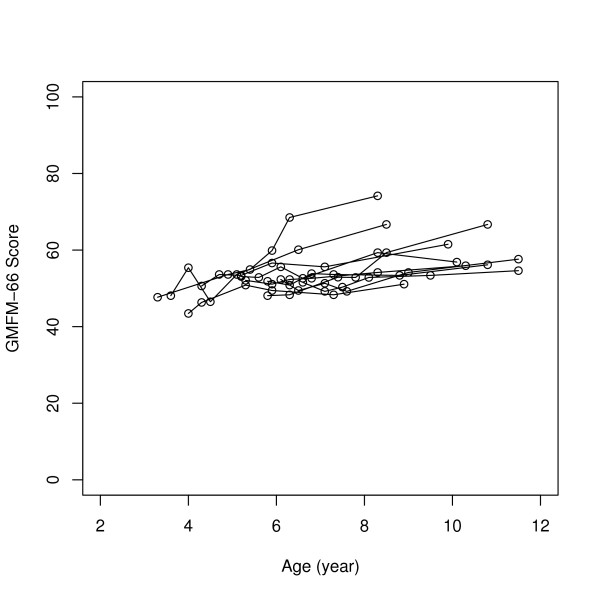
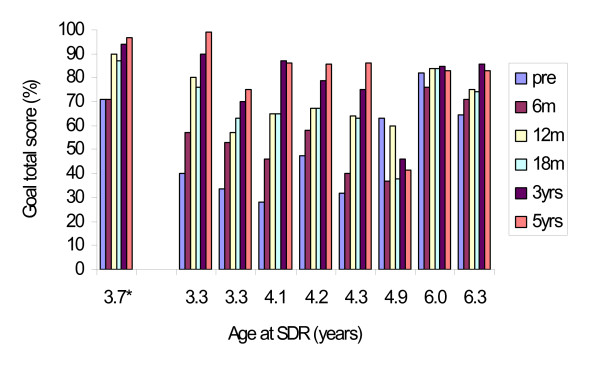
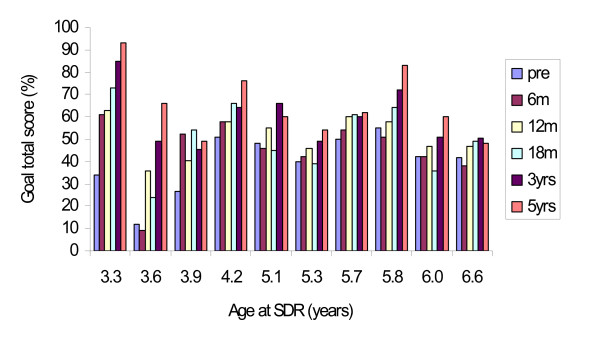
Methods: This study group consisted of 35 children, consecutively operated, with spastic diplegia, of which 26 were Gross Motor Function Classification System (GMFCS) levels III-V. Mean age was 4.5 years (range 2.5-6.6). They were all assessed by the same multidisciplinary team at pre- and at 6, 12, 18 months, 3 and 5 years postoperatively. Clinical and demographic data, complications and number of rootlets cut were prospectively registered. Deep tendon reflexes and muscle tone were examined, the latter graded with the modified Ashworth scale. Passive range of motion (PROM) was measured with a goniometer. Motor function was classified according to the GMFCS and measured with the Gross Motor Function Measure (GMFM-88) and derived into GMFM-66. Parent's opinions about the children's performance of skills and activities and the amount of caregiver assistance were measured with Pediatric Evaluation Disability Inventory (PEDI).
Results: The mean proportion of rootlets cut in S2-L2 was 40%. Muscle tone was immediately reduced in adductors, hamstrings and dorsiflexors (p < 0.001) with no recurrence of spasticity over the 5 years. For GMFCS-subgroups I-II, III and IV-V significant improvements during the five years were seen in PROM for hip abduction, popliteal angle and ankle dorsiflexion (p = 0.001), capacity of gross motor function (GMFM) (p = 0.001), performance of functional skills and independence in self-care and mobility (PEDI) (p = 0.001).
Conclusion: SDR is a safe and effective method for reducing spasticity permanently without major negative side effects. In combination with physiotherapy, in a group of carefully selected and systematically followed young children with spastic diplegia, it provides lasting functional benefits over a period of at least five years postoperatively.
Figures


References
-
- Westbom L, Hägglund G, Lundkvist A, Nordmark E, Strömblad L-G. New treament methods for spasticity and dystonia in children with cerebral palsy dictate multidisciplinary teamwork. Comprehensive approach yields good results. Lakartidningen. 2003;100:125–130. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
