

Inflammation and the host response to injury, a large-scale collaborative project: patient-oriented research core--standard operating procedures for clinical care VII--Guidelines for antibiotic administration in severely injured patients
- PMID: 19077651
- PMCID: PMC4004064
- DOI: 10.1097/TA.0b013e318184ee35
Inflammation and the host response to injury, a large-scale collaborative project: patient-oriented research core--standard operating procedures for clinical care VII--Guidelines for antibiotic administration in severely injured patients
Abstract
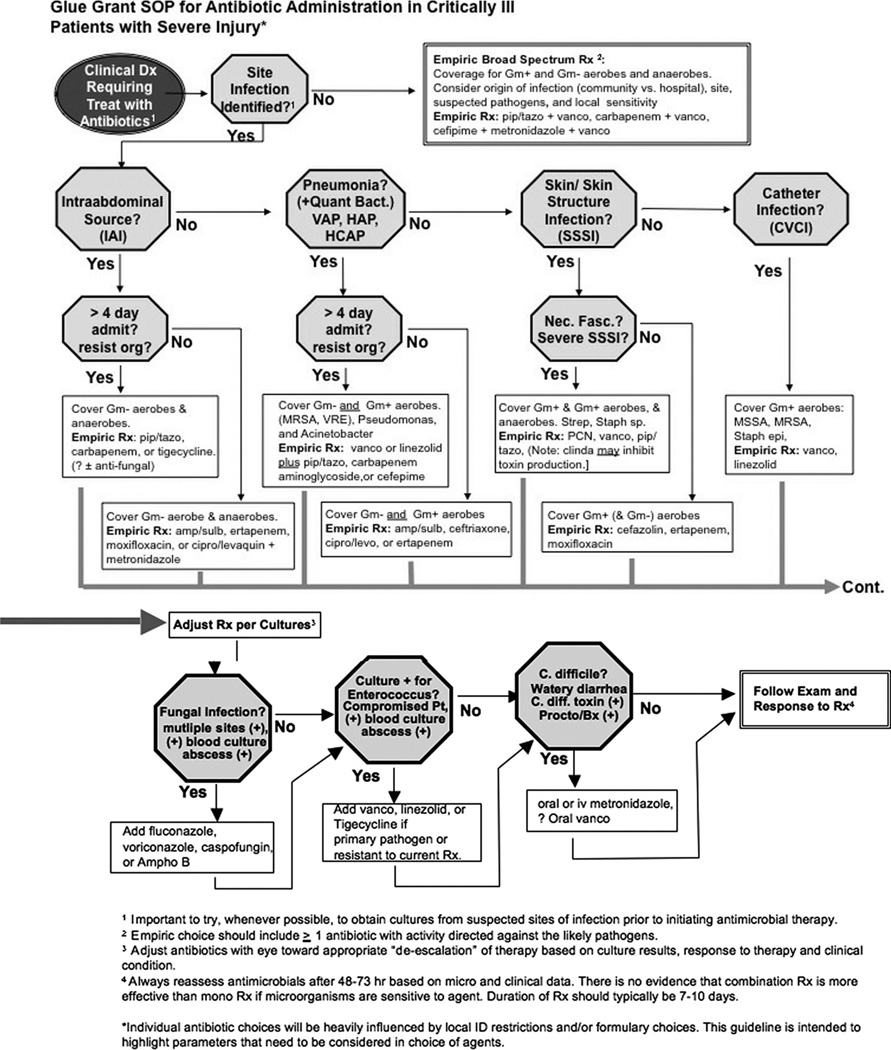
When the clinical decision to treat a critically ill patient with antibiotics has been made, one must attempt to identify the site of infection based on clinical signs and symptoms, laboratory or diagnostic radiology studies. Identification of site requires, examination of patient, inspection of all wounds, chest radiograph, and calculation of clinical pulmonary infection score if ventilated, obtaining blood cultures, urinalysis, and line change if clinical suspicion of central venous catheter (CVC) source. If it is impossible to identify site, obtain cultures from all accessible suspected sites and initiate empiric, broad spectrum antibiotics. If likely site can be identified answer these questions: Is intra-abdominal site suspected? Is pulmonary source of infection suspected? Is skin, skin structure or soft tissue site suspected? If yes, does the patient have clinical signs suspicion for necrotizing soft tissue infection (NSTI)? Is a CVC infection suspected? Risk factors for more complicated infections are discussed and specific antibiotic recommendations are provided for each type and severity of clinical infection. Decision to continue, discontinue and/or alter antibiotic/antimicrobial treatment should be based on the clinical response to treatment, diagnostic or interventional findings, and culture and sensitivity data, bearing in mind that not all patients with infections will have positive cultures because of limitations of specimen handling, microbiology laboratory variations, time between specimen acquisition and culture, or presence of effective antibiotics at the time that specimens were obtained. It should also be noted that not all patients with increased temperature/WBC have an infection. Discontinuation of antibiotics is appropriate if cultures and other diagnostic studies are negative.
Figures
References
-
- Ortiz R, Lee K. Nosocomial infections in neurocritical care. Curr Neurol Neurosci Rep. 2006;6:525–530. - PubMed
-
- Jaeger M, Maier D, Kern WV, Sudkamp NP. Antibiotics in trauma and orthopedic surgery—a primer of evidence-based recommendations. Injury. 2006;37(Suppl 2):S74–S80. - PubMed
-
- Dellit TH, Owens RC, McGowan JE, Jr, et al. Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America guidelines for developing an institutional program to enhance antimicrobial stewardship. Clin Infect Dis. 2007;44:159–177. - PubMed
-
- Chatterjee I, Iredell JR, Woods M, Lipman J. The implications of enterococci for the intensive care unit. Crit Care Resusc. 2007;9:69–75. - PubMed
-
- Merlino JI, Yowler CJ, Malangoni MA. Nosocomial infections adversely affect the outcomes of patients with serious intraabdominal infections. Surg Infect (Larchmt) 2004;5:21–27. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
