

Experimental validation of peptide immunohistochemistry controls
- PMID: 19077907
- PMCID: PMC2672113
- DOI: 10.1097/PAI.0b013e3181904379
Experimental validation of peptide immunohistochemistry controls
Abstract
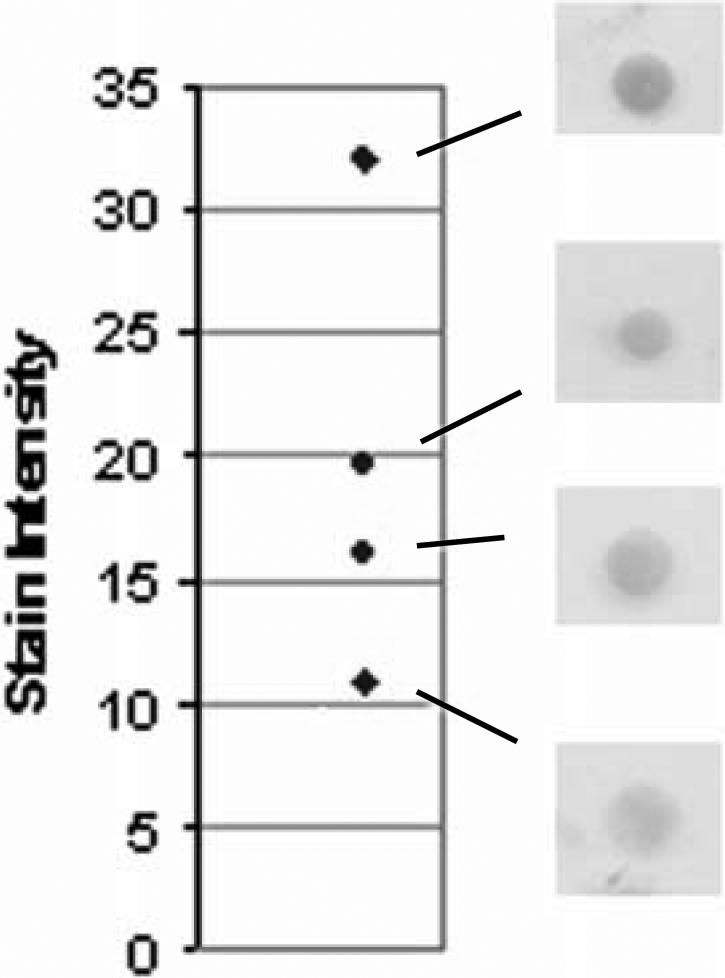
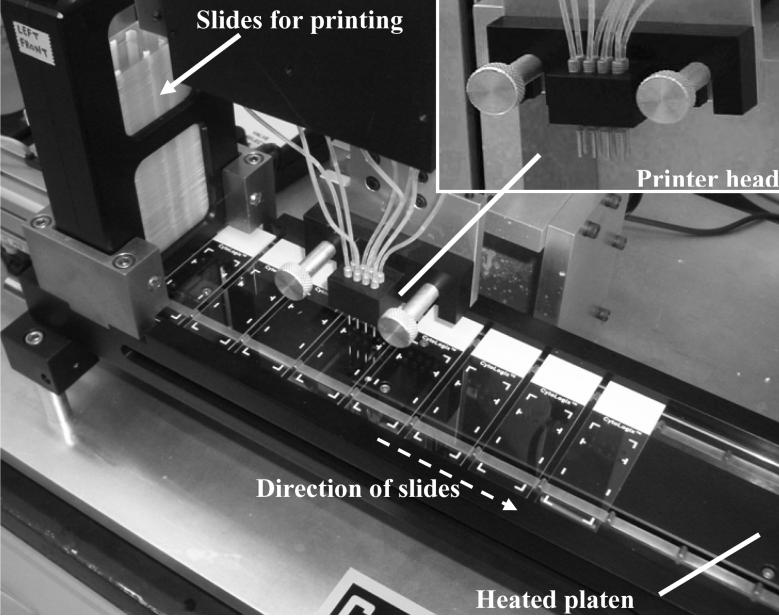
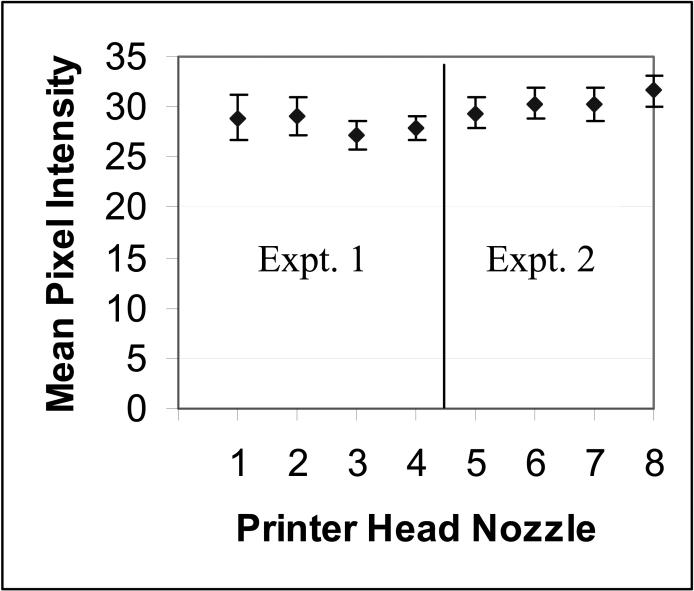
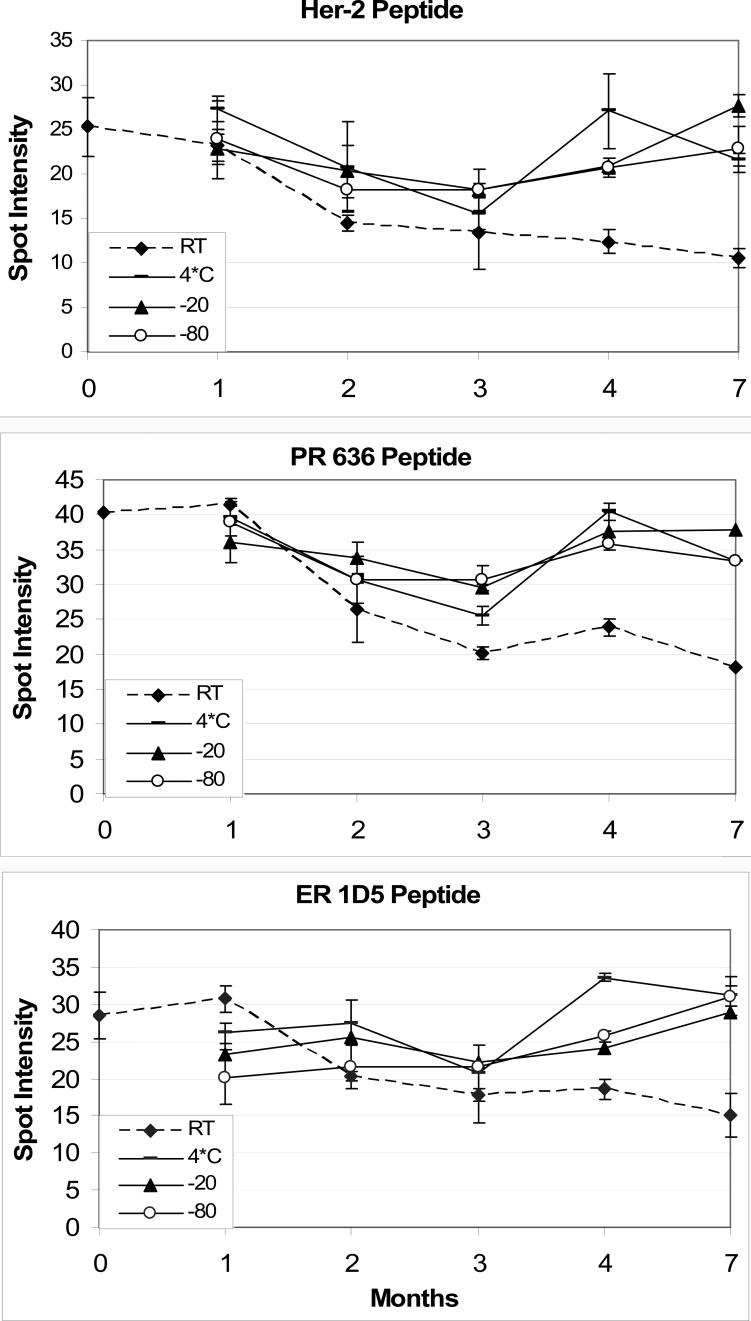
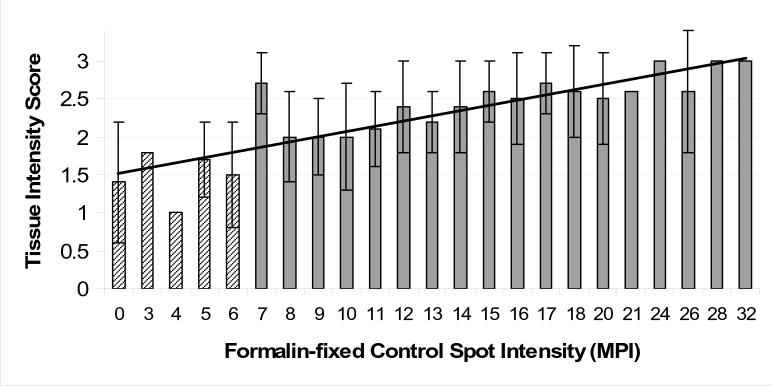
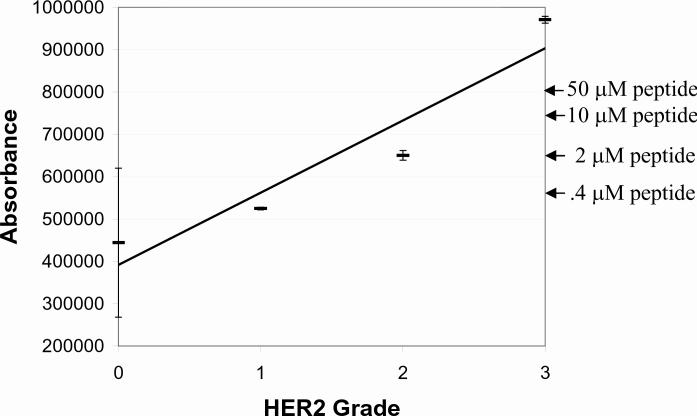
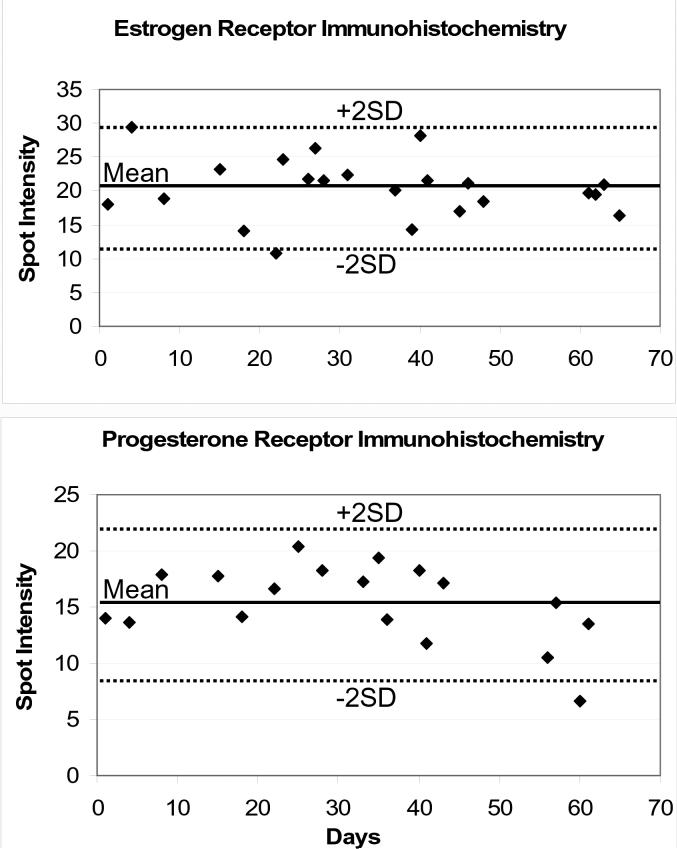
Peptide immunohistochemistry (IHC) controls are a new quality control format for verifying proper IHC assay performance, offering advantages in high throughput automated manufacture and standardization. We previously demonstrated that formalin-fixed peptide epitopes, covalently attached to glass microscope slides, behaved (immunochemically) in a similar fashion to the native protein in tissue sections. To convert this promising idea into a practical clinical laboratory quality control tool, we tested the hypothesis that the quality assurance information provided by peptide IHC controls accurately reflects IHC staining performance among a diverse group of clinical laboratories. To test the hypothesis, we first designed and built an instrument for reproducibly printing the controls on microscope slides and a simple software program to measure the color intensity of stained controls. Automated printing of peptide spots was reproducible, with coefficients of variation of 4% to 8%. Moreover, the peptide controls were stable at <or=4 degrees C for at least 7 months, the longest time duration we tested. A national study of 109 participating clinical laboratories demonstrated a good correlation between a laboratory's ability to properly stain formalin-fixed peptide controls to their ability in properly staining a 3+ HER-2 formalin-fixed tissue section mounted on the same slide (r=0.87). Therefore, peptide IHC controls accurately reflect the analytical component of an IHC stain, including antigen retrieval. Besides its use in proficiency survey testing, we also demonstrate the feasibility of applying peptide IHC controls for verifying intralaboratory IHC staining consistency, using Levy-Jennings charting.
Figures

References
-
- Paik S, Bryant J, Tan-Chiu E, et al. Real-world performance of HER2 testing -National Surgical Adjuvant Breast and Bowel Project experience. J. Natl. Cancer Inst. 2002;94(11):852–854. - PubMed
-
- Perez E, Suman V, Davidson N, et al. HER2 testing by local, central, and reference laboratories in specimens from the North Central Cancer Treatment Group N9831 Intergroup adjuvant trial. J Clin Oncol. 2006;24(19):3032–3038. - PubMed
-
- Roche P, Suman V, Jenkins R, et al. Concordance between local and central laboratory HER2 testing in the breast intergroup trial N9831. J Natl Cancer Inst. 2002;94:855–857. - PubMed
-
- Wolff A, Hammond M, Schwartz J, et al. American Society of Clinical Oncology/College of American Pathologists guideline recommendations for Human Epidermal Growth Factor Receptor 2 testing in breast cancer. Arch. Pathol. & Lab. Med. 2007;131:18–43. - PubMed
-
- Chung G, Zerkowski M, Ghosh S, Camp R, Rimm D. Quantitative analysis of estrogen receptor heterogeneity in breast cancer. Lab Invest. 2007;87(7):662–669. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
