

Placental endoplasmic reticulum stress and oxidative stress in the pathophysiology of unexplained intrauterine growth restriction and early onset preeclampsia
- PMID: 19081132
- PMCID: PMC2684656
- DOI: 10.1016/j.placenta.2008.11.003
Placental endoplasmic reticulum stress and oxidative stress in the pathophysiology of unexplained intrauterine growth restriction and early onset preeclampsia
Abstract
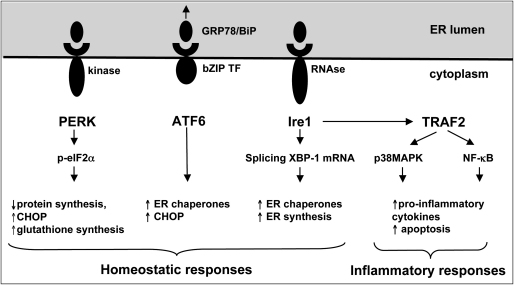
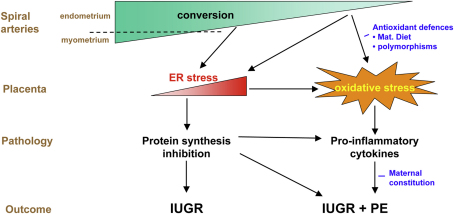
The pregnancy complications of unexplained intrauterine growth restriction and early onset preeclampsia are thought to share a common aetiology in placental malperfusion secondary to deficient maternal spiral artery conversion. A key question is whether the contrasting clinical manifestations reflect different placental pathologies, or whether they are due to altered maternal responses to a common factor derived from the placenta. Recently, molecular evidence of protein synthesis inhibition secondary to endoplasmic reticulum stress has provided an explanation for the small placental phenotype in both conditions. However, other pathways activated by more severe endoplasmic reticulum stress are only observed in placentas from pregnancies associated with early onset preeclampsia. Here, we review the literature and conclude that there is evidence of greater maternal vascular compromise of the placenta in these cases. We speculate that in cases of normotensive intrauterine growth restriction the placental pathology is centred predominantly around endoplasmic reticulum stress, whereas in cases complicated by preeclampsia oxidative stress is further superimposed. This causes the release of a potent mix of pro-inflammatory cytokines, anti-angiogenic factors and trophoblastic aponecrotic debris into the maternal circulation that causes the peripheral syndrome. Maternal and fetal constitutional factors may modulate how the placenta responds to the maternal vascular insult, and how the mother is affected by the placental factors released. However, the principal conclusion is that the difference between these two conditions lies in the severity of the initiating deficit in spiral arterial conversion, and the relative degrees of endoplasmic reticulum stress and oxidative stress induced in the placenta as a result.
Figures
References
-
- Ness R.B., Sibai B.M. Shared and disparate components of the pathophysiologies of fetal growth restriction and preeclampsia. Am J Obstet Gynecol. 2006;195:40–49. - PubMed
-
- Brosens I., Dixon H.G., Robertson W.B. Fetal growth retardation and the arteries of the placental bed. Br J Obstet Gynaecol. 1977;84:656–663. - PubMed
-
- Gerretsen G., Huisjes H.J., Elema J.D. Morphological changes of the spiral arteries in the placental bed in relation to pre-eclampsia and fetal growth retardation. Br J Obstet Gynaecol. 1981;88:876–881. - PubMed
-
- Meekins J.W., Pijnenborg R., Hanssens M., McFadyen I.R., Van Assche F.A. A study of placental bed spiral arteries and trophoblast invasion in normal and severe pre-eclamptic pregnancies. Br J Obstet Gynaecol. 1994;101:669–674. - PubMed
-
- Lyall F. The human placental bed revisited. Placenta. 2002;23:555–562. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
