

Impact of preexisting circulating effector T cells on the outcome of ABO-incompatible adult LDLT
- PMID: 19082716
- PMCID: PMC7102009
- DOI: 10.1007/s10620-008-0618-y
Impact of preexisting circulating effector T cells on the outcome of ABO-incompatible adult LDLT
Abstract
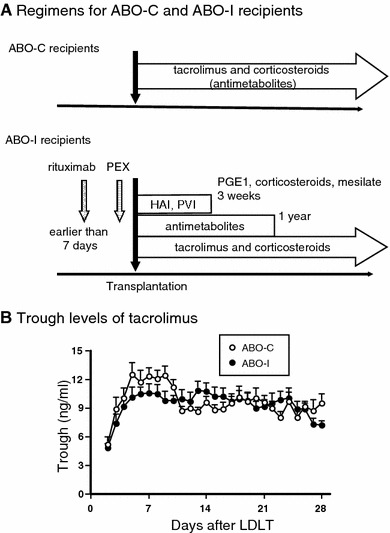
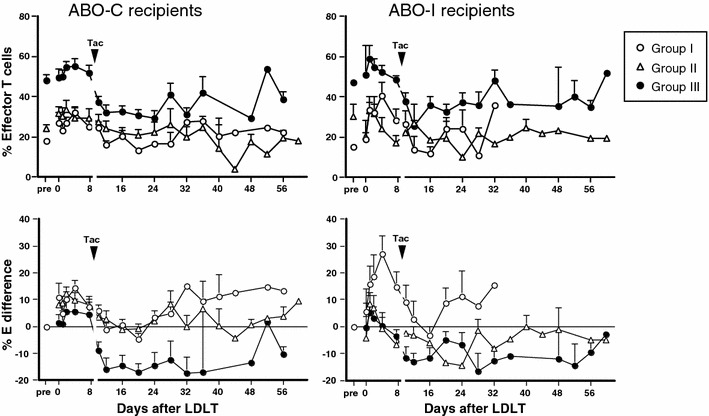
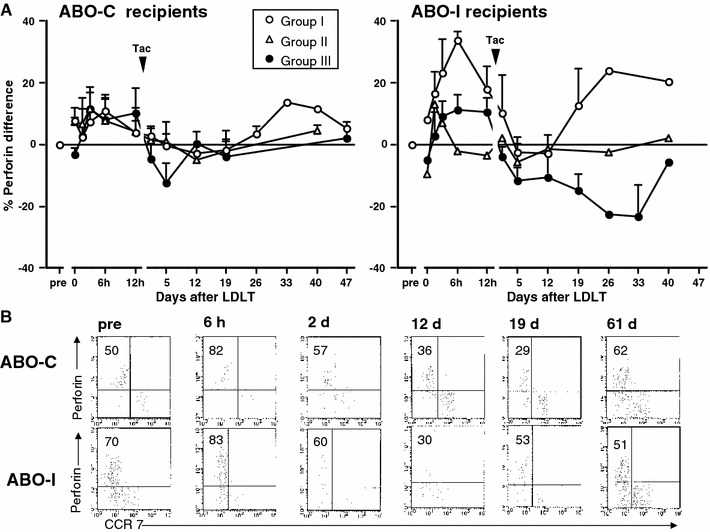
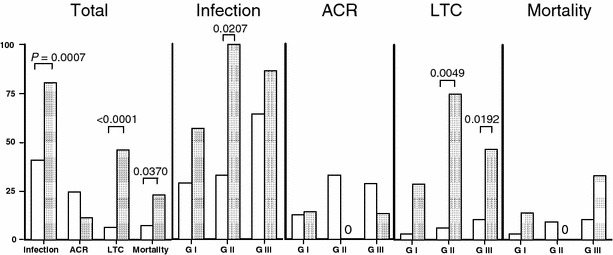
Our aim was to clarify the significance of phenotype of circulating CD8 T(+) cells on the outcome of ABO-incompatible (ABO-I) living donor liver transplantation (LDLT). Twenty-six recipients undergoing ABO-I LDLT and 92 undergoing ABO-compatible (ABO-C) LDLT were classified into three groups according to preoperative proportion of CD8 T(+) cells: naive-dominant (group I), effector memory-dominant (group II), and effector-dominant (group III) recipients. The clinical courses were analyzed. The results showed that in ABO-C groups I and II and in ABO-I group I, effector cells remained above the pretransplant levels after tacrolimus administration. However, in ABO-C group III and ABO-I groups II and III, effector cells were down-regulated for a prolonged period, along with markedly decreased perforin expression and frequent life-threatening complications. ABO-I group II and group III recipients had higher infection rates. It was concluded that recipients with preexisting high effector CD8 T(+) cells are unfavorable candidates for ABO-I LDLT.
Figures
References
-
- Hanto DW, Fecteau AH, Alonso MH, Valente JF, Whiting JF. ABO-incompatible liver transplantation with no immunological graft losses using total plasma exchange, splenectomy, and quadruple immunosuppression: evidence for accommodation. Liver Transpl. 2003;9(1):22–30. doi: 10.1053/jlts.2003.50011. - DOI - PubMed
-
- Welsh RM, Selin LK. No one is naive: the significance of heterologous T cell immunity. Nat Rev Immunol. 2002;2:417–426. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
