

A level-1 pilot study to evaluate of ultraporous beta-tricalcium phosphate as a graft extender in the posterior correction of adolescent idiopathic scoliosis
- PMID: 19082847
- PMCID: PMC2899343
- DOI: 10.1007/s00586-008-0844-1
A level-1 pilot study to evaluate of ultraporous beta-tricalcium phosphate as a graft extender in the posterior correction of adolescent idiopathic scoliosis
Abstract
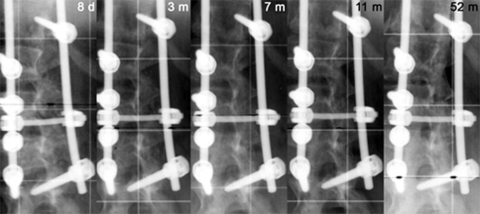
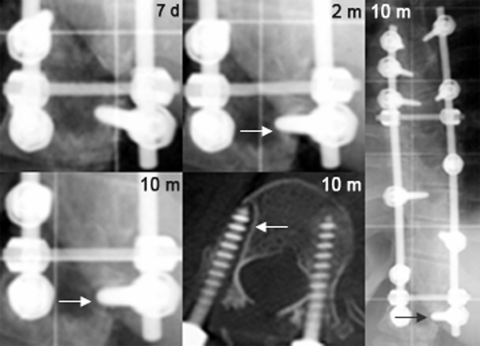
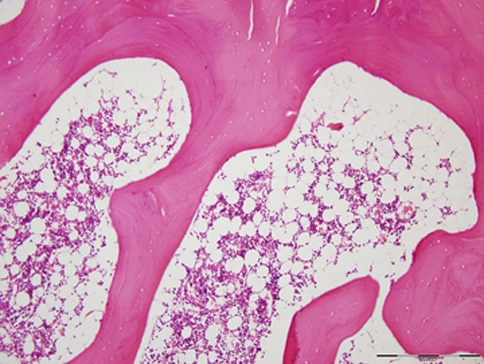
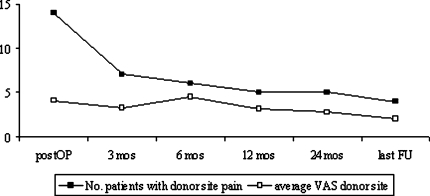
The objective of this study is to compare the clinical and radiographic results of ultraporous beta-tricalcium phosphate (beta-TCP) versus autogenous iliac crest bone graft (ICBG), through prospective randomized pilot study (EBM-Level 1), as graft extenders in scoliosis surgery. In the posterior correction of scoliosis, local bone resected as part of the procedure is used as the base bone graft material. Supplemental grafting from the iliac crest is considered the gold-standard in posterior spinal fusion. However, autograft is not available in unlimited quantities, and bone harvesting is a source of significant morbidity. Ultraporous beta-TCP might be a substitute for ICBG in these patients and thus eliminate donor site morbidity. A total of 40 patients with adolescent idiopathic scoliosis (AIS) were randomized into two treatment groups and underwent corrective posterior instrumentation. In 20 patients, ICBG harvesting was performed whereas the other half received beta-TCP (VITOSS) to augment the local bone graft. If thoracoplasty was performed, the resected rib bone was added in both groups. Patients were observed clinically and radiographically for a minimum of 20 months postoperatively, with a mean follow-up of 4 years. Overall pain and pain specific to the back and donor site were assessed using a visual analog scale (VAS). As a result, both groups were comparable with respect to the age at the time of surgery, gender ratio, preoperative deformity, and hence length of instrumentation. There was no significant difference in blood loss and operative time. In nine patients of the beta-TCP group and eight patients of the ICBG group, thoracoplasty was performed resulting in a rib graft of on average 7.9 g in both groups. Average curve correction was 61.7% in the beta-TCP group and 61.2% in the ICBG group at hospital discharge (P=0.313) and 57.2 and 54.3%, respectively, at follow-up (P=0.109). Loss of curve correction amounted on average 2.6 degrees in the beta-TCP group and 4.2 degrees in the comparison group (P=0.033). In the ICBG group, four patients still reported donor site pain of on average 2/10 on the VAS at last follow-up. One patient in the beta-TCP group was diagnosed with a pseudarthrosis at the caudal end of the instrumentation. Revision surgery demonstrated solid bone formation directly above the pseudarthrosis with no histological evidence of beta-TCP in the biopsy taken. In conclusion, the use of beta-TCP instead of ICBG as extenders of local bone graft yielded equivalent results in the posterior correction of AIS. The promising early results of this pilot study support that beta-TCP appears to be an effective bone substitute in scoliosis surgery avoiding harvesting of pelvic bone and the associated morbidity.
Figures

Similar articles
-
Silicate-substituted calcium phosphate as a bone graft substitute in surgery for adolescent idiopathic scoliosis.Eur Spine J. 2013 Mar;22 Suppl 2(Suppl 2):S185-94. doi: 10.1007/s00586-012-2485-7. Epub 2012 Sep 5. Eur Spine J. 2013. PMID: 22948551 Free PMC article. Clinical Trial.
-
Adjunctive use of ultraporous beta-tricalcium phosphate bone void filler in spinal arthrodesis.Orthopedics. 2002 May;25(5 Suppl):s579-84. doi: 10.3928/0147-7447-20020502-06. Orthopedics. 2002. PMID: 12038845
-
Influence of 45S5 Bioactive Glass in A Standard Calcium Phosphate Collagen Bone Graft Substitute on the Posterolateral Fusion of Rabbit Spine.Iowa Orthop J. 2017;37:193-198. Iowa Orthop J. 2017. PMID: 28852357 Free PMC article.
-
Bone graft in posterior spine fusion for adolescent idiopathic scoliosis: a meta-analysis.ANZ J Surg. 2018 Dec;88(12):1247-1252. doi: 10.1111/ans.14551. Epub 2018 May 15. ANZ J Surg. 2018. PMID: 29763982 Review.
-
Guideline update for the performance of fusion procedures for degenerative disease of the lumbar spine. Part 16: bone graft extenders and substitutes as an adjunct for lumbar fusion.J Neurosurg Spine. 2014 Jul;21(1):106-32. doi: 10.3171/2014.4.SPINE14325. J Neurosurg Spine. 2014. PMID: 24980593 Review.
Cited by
-
Settable Polymeric Autograft Extenders in a Rabbit Radius Model of Bone Formation.Materials (Basel). 2021 Jul 15;14(14):3960. doi: 10.3390/ma14143960. Materials (Basel). 2021. PMID: 34300888 Free PMC article.
-
Preliminary study showing safety/efficacy of nanoss bioactive versus vitoss as bone graft expanders for lumbar noninstrumented fusions.Surg Neurol Int. 2015 Jun 25;6(Suppl 10):S318-22. doi: 10.4103/2152-7806.159380. eCollection 2015. Surg Neurol Int. 2015. PMID: 26167369 Free PMC article.
-
Anterior cervical arthrodesis using an osteoconductive scaffold: The use of beta-tricalcium phosphate with local bone marrow aspirate in over 100 patients.SAS J. 2009 Sep 1;3(3):114-7. doi: 10.1016/j.esas.2009.09.008. eCollection 2009. SAS J. 2009. PMID: 25802636 Free PMC article. No abstract available.
-
Bone substitutes and expanders in Spine Surgery: A review of their fusion efficacies.Int J Spine Surg. 2016 Sep 22;10:33. doi: 10.14444/3033. eCollection 2016. Int J Spine Surg. 2016. PMID: 27909654 Free PMC article.
-
Preliminary documentation of the comparable efficacy of vitoss versus NanOss bioactive as bone graft expanders for posterior cervical fusion.Surg Neurol Int. 2015 May 7;6(Suppl 4):S164-71. doi: 10.4103/2152-7806.156559. eCollection 2015. Surg Neurol Int. 2015. PMID: 26005578 Free PMC article.
References
-
- Aurori BF, Weierman RJ, Lowell HA, et al. Pseudarthrosis after spinal fusion for scoliosis. A comparison of autogeneic and allogeneic bone grafts. Clin Orthop Relat Res. 1985;199:153–153. - PubMed
-
- Betz RR. Limitations of autograft and allograft: new synthetic solutions. Orthopedics. 2002;25:s561–s570. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
