

Biallelic somatic and germline mutations in cerebral cavernous malformations (CCMs): evidence for a two-hit mechanism of CCM pathogenesis
- PMID: 19088123
- PMCID: PMC2640209
- DOI: 10.1093/hmg/ddn430
Biallelic somatic and germline mutations in cerebral cavernous malformations (CCMs): evidence for a two-hit mechanism of CCM pathogenesis
Abstract
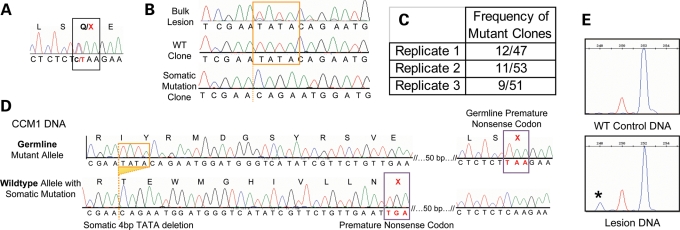
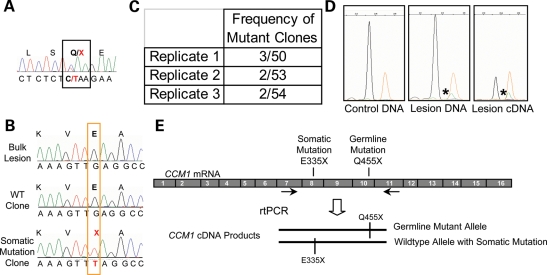
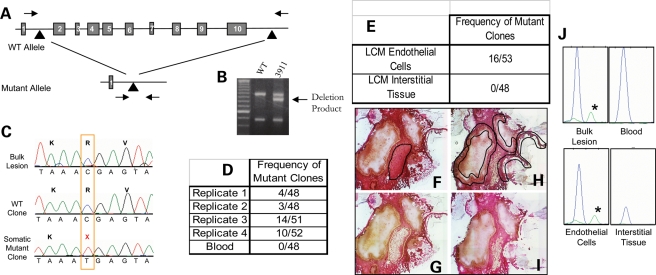
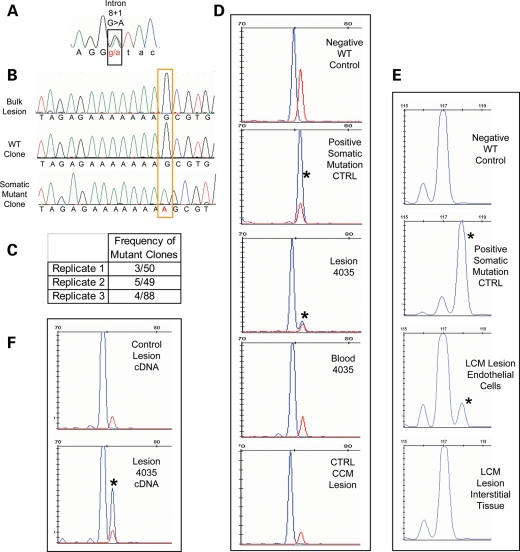
Cerebral cavernous malformations (CCMs) are vascular anomalies of the central nervous system, comprising dilated blood-filled capillaries lacking structural support. The lesions are prone to rupture, resulting in seizures or hemorrhagic stroke. CCM can occur sporadically, manifesting as solitary lesions, but also in families, where multiple lesions generally occur. Familial cases follow autosomal-dominant inheritance due to mutations in one of three genes, CCM1/KRIT1, CCM2/malcavernin or CCM3/PDCD10. The difference in lesion burden between familial and sporadic CCM, combined with limited molecular data, suggests that CCM pathogenesis may follow a two-hit molecular mechanism, similar to that seen for tumor suppressor genes. In this study, we investigate the two-hit hypothesis for CCM pathogenesis. Through repeated cycles of amplification, subcloning and sequencing of multiple clones per amplicon, we identify somatic mutations that are otherwise invisible by direct sequencing of the bulk amplicon. Biallelic germline and somatic mutations were identified in CCM lesions from all three forms of inherited CCMs. The somatic mutations are found only in a subset of the endothelial cells lining the cavernous vessels and not in interstitial lesion cells. These data suggest that CCM lesion genesis requires complete loss of function for one of the CCM genes. Although widely expressed in the different cell types of the brain, these data also suggest a unique role for the CCM proteins in endothelial cell biology.
Figures
References
-
- Rigamonti D., Hadley M.N., Drayer B.P., Johnson P.C., Hoenig-Rigamonti K., Knight J.T., Spetzler R.F. Cerebral cavernous malformations. Incidence and familial occurrence. N. Engl. J. Med. 1988;319:343–347. - PubMed
-
- Gault J., Sarin H., Awadallah N.A., Shenkar R., Awad I.A. Pathobiology of human cerebrovascular malformations: basic mechanisms and clinical relevance. Neurosurgery. 2004;55:1–16. discussion 16–17. - PubMed
-
- Laberge-le Couteulx S., Jung H.H., Labauge P., Houtteville J.P., Lescoat C., Cecillon M., Marechal E., Joutel A., Bach J.F., Tournier-Lasserve E. Truncating mutations in CCM1, encoding KRIT1, cause hereditary cavernous angiomas. Nat. Genet. 1999;23:189–193. - PubMed
-
- Sahoo T., Johnson E.W., Thomas J.W., Kuehl P.M., Jones T.L., Dokken C.G., Touchman J.W., Gallione C.J., Lee-Lin S.Q., Kosofsky B., et al. Mutations in the gene encoding KRIT1, a Krev-1/rap1a binding protein, cause cerebral cavernous malformations (CCM1) Hum. Mol. Genet. 1999;8:2325–2333. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
