

Treatment response to transcatheter arterial embolization and chemoembolization in primary and metastatic tumors of the liver
- PMID: 19088924
- PMCID: PMC2597318
- DOI: 10.1080/13651820802356564
Treatment response to transcatheter arterial embolization and chemoembolization in primary and metastatic tumors of the liver
Abstract
Introduction: Transcatheter arterial embolization (TAE) and chemoembolization (TACE) are increasingly used to treat unresectable primary and metastatic liver tumors. The purpose of this study was to determine the objective response to TAE and TACE in unresectable hepatic malignancies and to identify clinicopathologic predictors of response.
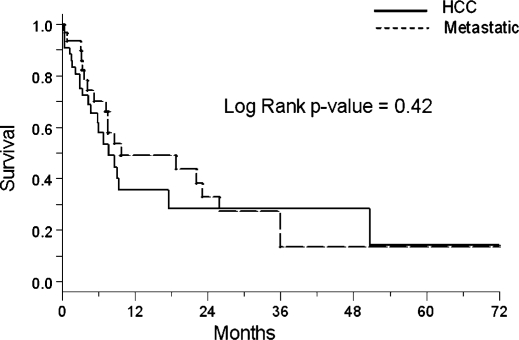
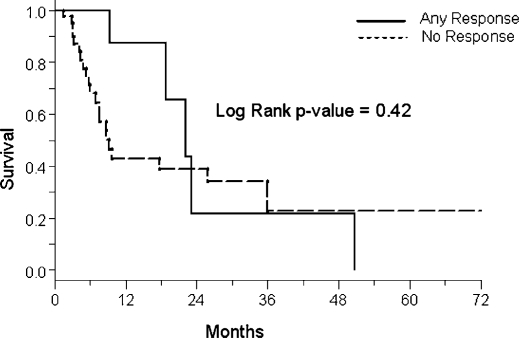
Materials and methods: Seventy-nine consecutive patients who underwent 119 TAE/TACE procedures between 1998 and 2006 were reviewed. The change in maximal diameter of 121 evaluable lesions in 56 patients was calculated from pre and post-procedure imaging. Response rates were determined using Response Evaluation Criteria in Solid Tumors (RECIST) guidelines. The Kaplan-Meier method was used to compare survival in responders vs. non-responders and in primary vs. metastatic histologies.
Results: TAE and TACE resulted in a mean decrease in lesion size of 10.3%+/-1.9% (p<0.001). TACE (vs. TAE) and carcinoid tumors were associated with a greater response (p<0.05). Lesion response was not predicted by pre-treatment size, vascularity, or histology. The RECIST partial response (PR) rate was 12.3% and all partial responders were in the TACE group. Neuroendocrine tumors, and specifically carcinoid lesions, had a significantly greater PR rate (p<0.05). Overall survival, however, was not associated with histology or radiologic response.
Discussion: TAE and TACE produce a significant objective treatment response by RECIST criteria. Response is greatest in neuroendocrine tumors and is independent of vascularity and lesion size. TACE appears to be superior to TAE. Although an association of response with improved survival was not demonstrated, large cohort studies are necessary to further define this relationship.
Keywords: RECIST; chemoembolization; regional therapy.
Figures
Similar articles
-
Radiofrequency ablation combined with transcatheter therapy in rabbit VX2 liver tumors: effects and histopathological characteristics.Acta Radiol. 2015 Jan;56(1):87-96. doi: 10.1177/0284185113520266. Epub 2014 Jan 14. Acta Radiol. 2015. PMID: 24425792
-
A comparative study between Embosphere(®) and conventional transcatheter arterial chemoembolization for treatment of unresectable liver metastasis from GIST.Chin J Cancer Res. 2014 Feb;26(1):124-31. doi: 10.3978/j.issn.1000-9604.2014.02.11. Chin J Cancer Res. 2014. PMID: 24653635 Free PMC article.
-
Hepatic artery embolization in advanced neuroendocrine tumors: Efficacy and long-term outcomes.Asia Pac J Clin Oncol. 2016 Mar;12(1):61-9. doi: 10.1111/ajco.12438. Epub 2015 Dec 14. Asia Pac J Clin Oncol. 2016. PMID: 26663886
-
Transarterial (chemo)embolisation versus no intervention or placebo for liver metastases.Cochrane Database Syst Rev. 2020 Mar 12;3(3):CD009498. doi: 10.1002/14651858.CD009498.pub4. Cochrane Database Syst Rev. 2020. PMID: 32163181 Free PMC article.
-
The clinical safety and efficacy of conventional transcatheter arterial chemoembolization and drug-eluting beads-transcatheter arterial chemoembolization for unresectable hepatocellular carcinoma: A meta-analysis.Biosci Trends. 2019 Nov 13;13(5):374-381. doi: 10.5582/bst.2019.01153. Epub 2019 Oct 14. Biosci Trends. 2019. PMID: 31611486 Review.
Cited by
-
Hepatic arterial therapy with drug-eluting beads in the management of metastatic pancreatic carcinoma to the liver: a multi-institutional registry.J Oncol. 2012;2012:168303. doi: 10.1155/2012/168303. Epub 2012 Feb 15. J Oncol. 2012. PMID: 22481917 Free PMC article.
-
Hepatic parenchymal changes following transcatheter embolization and chemoembolization in a rabbit tumor model.PLoS One. 2013 Aug 14;8(8):e70757. doi: 10.1371/journal.pone.0070757. eCollection 2013. PLoS One. 2013. PMID: 23967098 Free PMC article.
-
Adult Embryonal Sarcoma of the Liver: Management of a Massive Liver Tumor.Case Rep Surg. 2016;2016:5625762. doi: 10.1155/2016/5625762. Epub 2016 Nov 8. Case Rep Surg. 2016. PMID: 27895954 Free PMC article.
-
Short-term effectiveness of radiochemoembolization for selected hepatic metastases with a combination protocol.World J Gastroenterol. 2012 Oct 7;18(37):5249-59. doi: 10.3748/wjg.v18.i37.5249. World J Gastroenterol. 2012. PMID: 23066320 Free PMC article.
-
Utility of Core Biopsy Specimen to Identify Histologic Subtype and Predict Outcome for Lung Adenocarcinoma.Ann Thorac Surg. 2019 Aug;108(2):392-398. doi: 10.1016/j.athoracsur.2019.03.043. Epub 2019 Apr 12. Ann Thorac Surg. 2019. PMID: 30986416 Free PMC article.
References
-
- Llovet JM. Updated treatment approach to hepatocellular carcinoma. J Gastroenterol. 2005;40(3):225–35. - PubMed
-
- Liapi E, Geschwind JF. Transcatheter and ablative therapeutic approaches for solid malignancies. J Clin Oncol. 2007;25(8):978–86. - PubMed
-
- Stuart K. Chemoembolization in the management of liver tumors. Oncologist. 2003;8(5):425–37. - PubMed
-
- Sullivan KL. Hepatic artery chemoembolization. Semin Oncol. 2002;29(2):145–51. - PubMed
-
- Patt YZ, Chuang VP, Wallace S, Benjamin RS, Fuqua R, Mavligit GM. Hepatic arterial chemotherapy and occlusion for palliation of primary hepatocellular and unknown primary neoplasms in the liver. Cancer. 1983;51(8):1359–63. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
