

Striving for a better operative outcome: 101 pancreaticoduodenectomies
- PMID: 19088934
- PMCID: PMC2597329
- DOI: 10.1080/13651820802247094
Striving for a better operative outcome: 101 pancreaticoduodenectomies
Abstract
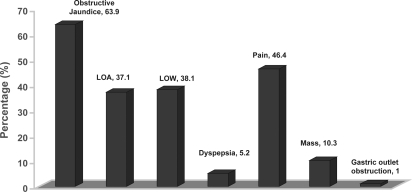
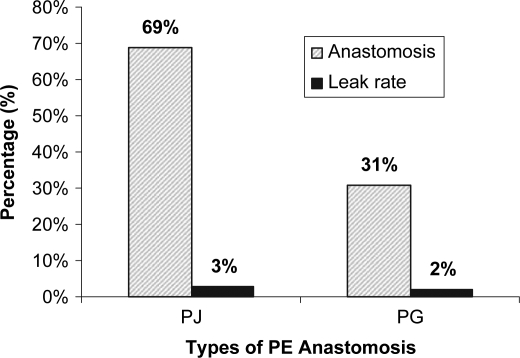
Pancreaticoduodenectomy (PD), once carried high morbidity and mortality, is now a routine operation performed for lesions arising from the pancreatico-duodenal complex. This study reviews the outcome of 101 pancreaticoduodenectomies performed after formalization of HepatoPancreatoBiliary (HPB) unit in the Department of Surgery. A prospective database comprising of patients who underwent PD was set up in 1999. Retrospective data for patients operated between 1996 and 1999 was included. One hundred and one cases accrued over 10 years from 1996 to 2006 were analysed using SPSS (Version 12.0). The mean age of our cohort of patients was 61+/-12 years with male to female ratio of 2:1. The commonest clinical presentations were obstructive jaundice (64%) and abdominal pain (47%). Majority had malignant lesions (86%) with invasive adenocarcinoma of the head of pancreas being the predominant histopathology (41%). Median operative time was 315 (180-945) minutes. Two-third of our patients had pancreaticojejunostomy (PJ) while the rest had pancreaticogastrostomy (PG). There were five patients with pancreatico-enteric anastomotic leak (5%), three of whom (3%) were from PJ anastomosis. Overall, in-hospital and 30-day mortality were both 3%. The median post-operative length of stay (LOS) was 15 days. Using logistic regressions, the post-operative morbidity predicts LOS following operation (p<0.005). The strategy in improving the morbidity and mortality rates of pancreaticoduodenectomies lies in the subspecialization of surgical services with regionalization of such complex surgeries to high volume centers. The key success lies in the dedication of staffs who continues to refine the clinical care pathway and standardize management protocol.
Keywords: Whipple operation; pancreaticoduodenectomy.
Figures
References
-
- Halsted WS. Contributions to the surgery of the bile passages, especially of the common bile duct. Boston Med Surg J. 1899;141:645–54.
-
- Pedrazzoli S, Beger HG, Obertop H, Andren-Sandberg A, Fernandez-Cruz L, Henne-Bruns D. A surgical and pathological based classification of resective treatment of pancreatic cancer. Summary of an international workshop on surgical procedures in pancreatic cancer. Dig Surg. 1999;16:337–45. - PubMed
LinkOut - more resources
Full Text Sources
