

Review
doi: 10.1007/s00247-008-1064-x.
Epub 2008 Dec 17.
Autosomal recessive polycystic kidney disease and congenital hepatic fibrosis (ARPKD/CHF)
Affiliations
- PMID: 19089418
- PMCID: PMC2918426
- DOI: 10.1007/s00247-008-1064-x
Item in Clipboard
Review
Autosomal recessive polycystic kidney disease and congenital hepatic fibrosis (ARPKD/CHF)
Pediatr Radiol.
2009 Feb.
Abstract
ARPKD/CHF is an inherited disease characterized by non-obstructive fusiform dilatation of the renal collecting ducts leading to enlarged spongiform kidneys and ductal plate malformation of the liver resulting in congenital hepatic fibrosis. ARPKD/CHF has a broad spectrum of clinical presentations involving the kidney and liver. Imaging plays an important role in the diagnosis and follow-up of ARPKD/CHF. Combined use of conventional and high-resolution US with MR cholangiography in ARPKD/CHF patients allows detailed definition of the extent of kidney and hepatobiliary manifestations without requiring ionizing radiation and contrast agents.
Figures
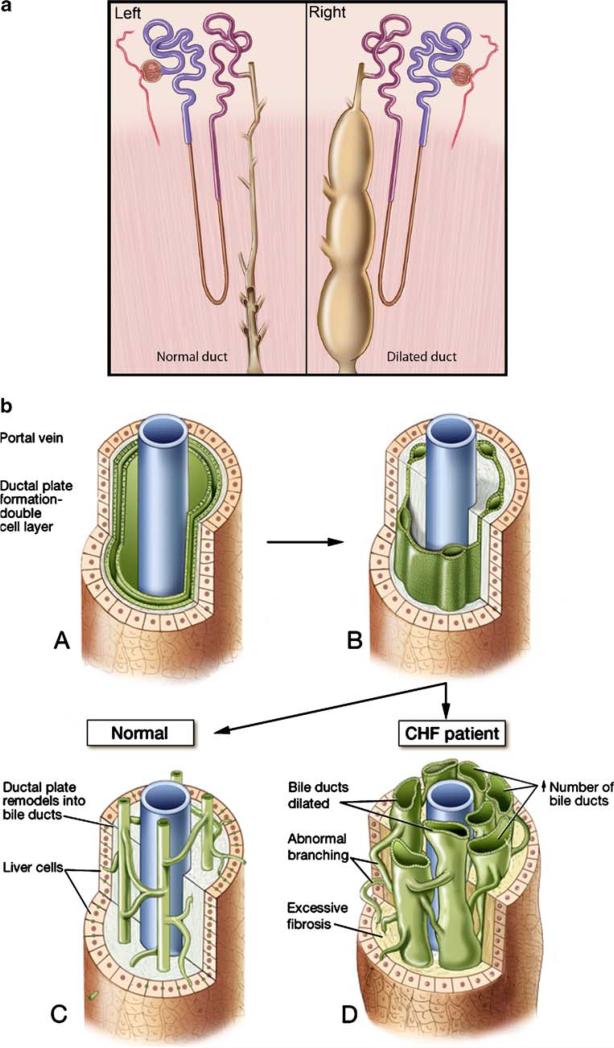
Normal and abnormal renal collecting ducts and biliary ductal plate. a Drawings demonstrate the normal structure of a renal collecting duct (left) and an abnormally dilated collecting duct of ARPKD (right). b The flow chart illustrates the normal development of the ductal plate from the double cell layer (A, B) to the bile ducts around the portal vein (C) and abnormal ductal plate remodeling (D), which results in dilated bile ducts with abnormal branching and fibrosis in CHF
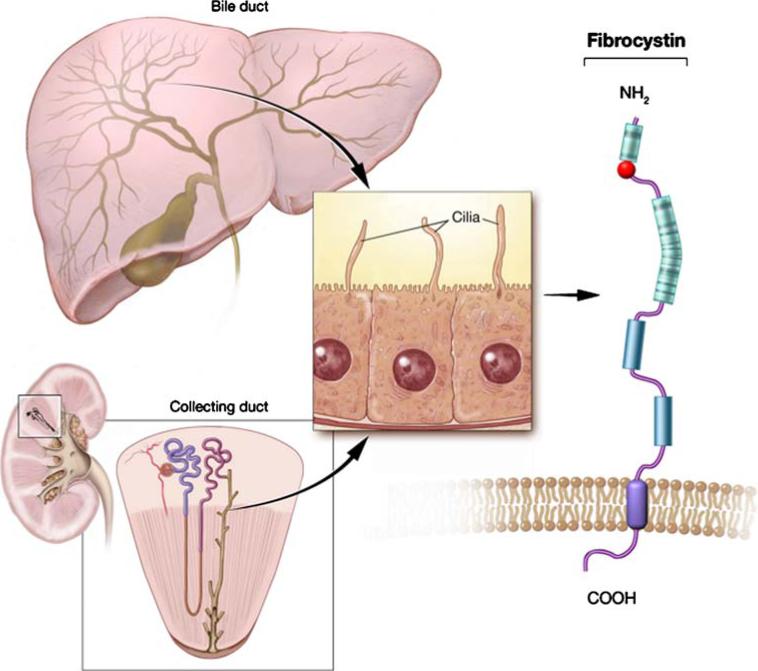
Diagram demonstrates the ultrastructure of the fibrocystin (polycystin) molecule, which is expressed in the cilia of both the bile ducts of the liver and collecting ducts of the kidney
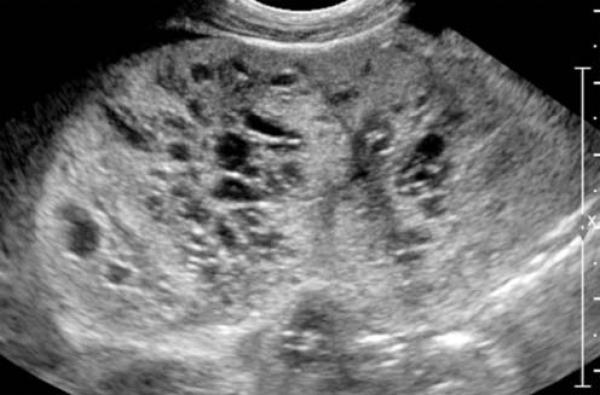
US image of a newborn with a perinatal ARPKD/CHF demonstrates an enlarged and diffusely echogenic right kidney secondary to numerous corticomedullary cysts (courtesy of Dr. Yair Anikster, Israel)
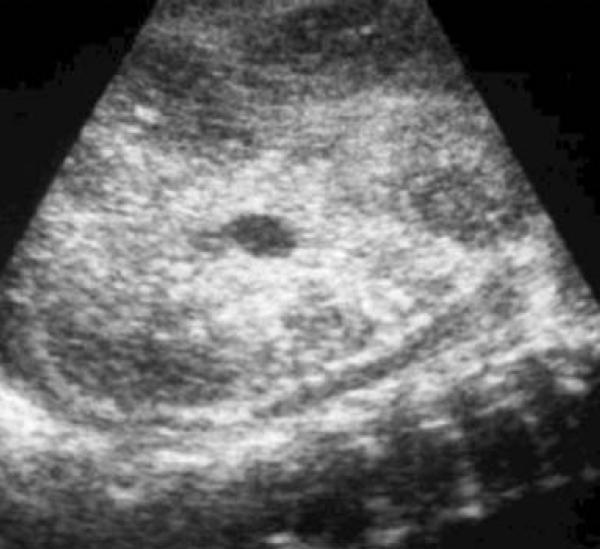
US image of a fetus with ARPKD/CHF demonstrates an enlarged echogenic right kidney (courtesy of Dr. Paula Woodward, University of Utah, Salt Lake City, UT)
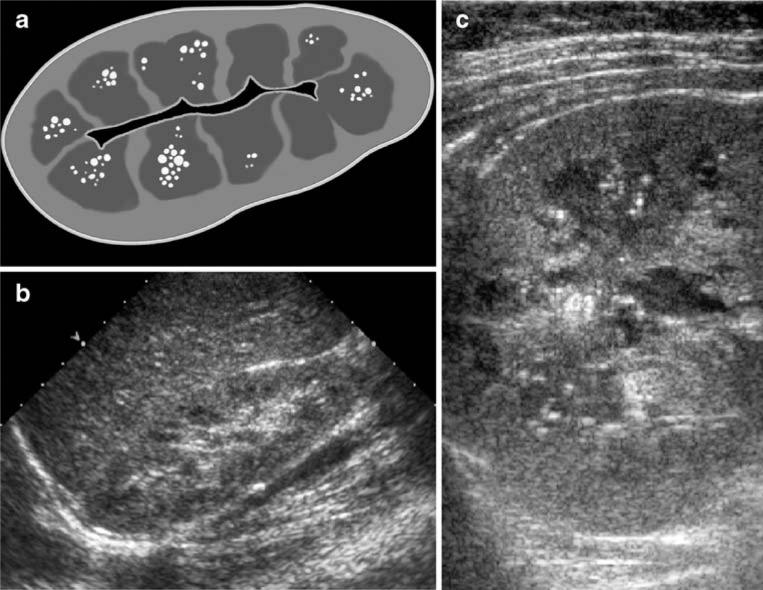
A 10-year-old girl with ARPKD/CHF. a Drawing represents partial medullary involvement in ARPKD. b Sagittal US image obtained with a conventional 4-MHz probe shows a normal-size right kidney with a preserved cortex and a mildly echogenic renal medulla. c High-resolution US image obtained with a 6-MHz probe demonstrates a few microcysts and echogenic foci within the medulla and a preserved renal cortex
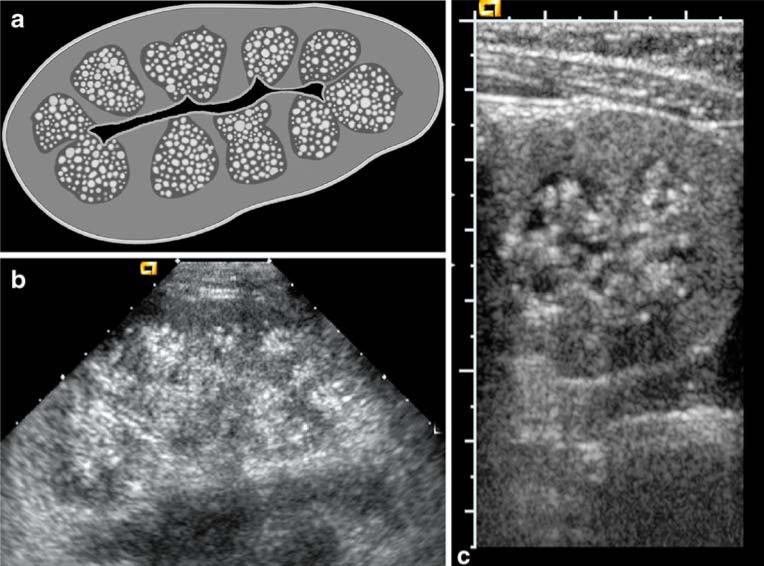
A 10-year-old boy with ARPKD/CHF. a Drawing represents complete medullary involvement in ARPKD. b Sagittal US image obtained with a conventional 4-MHz probe shows a mildly enlarged right kidney with a preserved cortex but significantly echogenic renal medulla. c High-resolution US image obtained with a 6-MHz probe demonstrates numerous microcysts and echogenic foci in the medulla with a preserved cortex
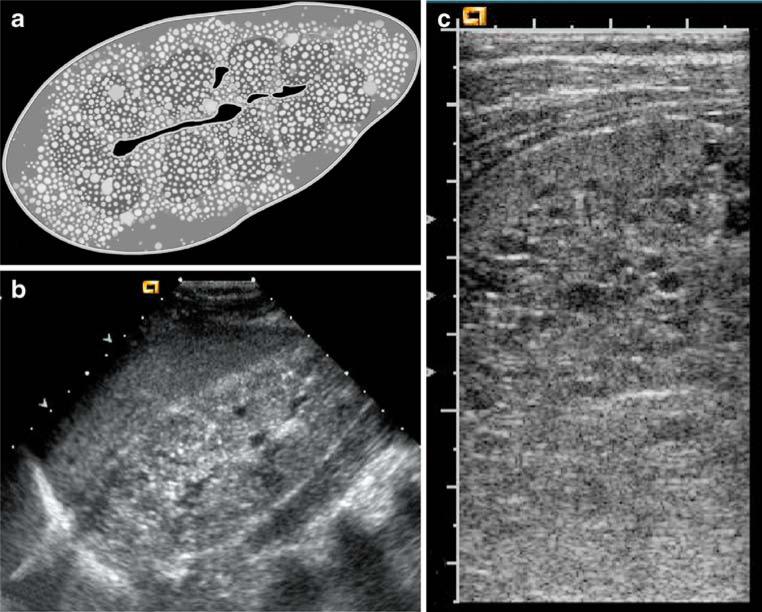
An 8-year-old boy with ARPKD/CHF. a Drawing represents complete medullary involvement with <50% partial cortical involvement in ARPKD. b Sagittal US image obtained with a conventional 4-MHz probe shows a diffuse moderately echogenic right kidney with mild corticomedullary distinction loss. c High-resolution US image obtained with a 6-MHz probe demonstrates numerous microcysts invading the entire medulla and partially invading the cortex (<50%) with a few echogenic foci
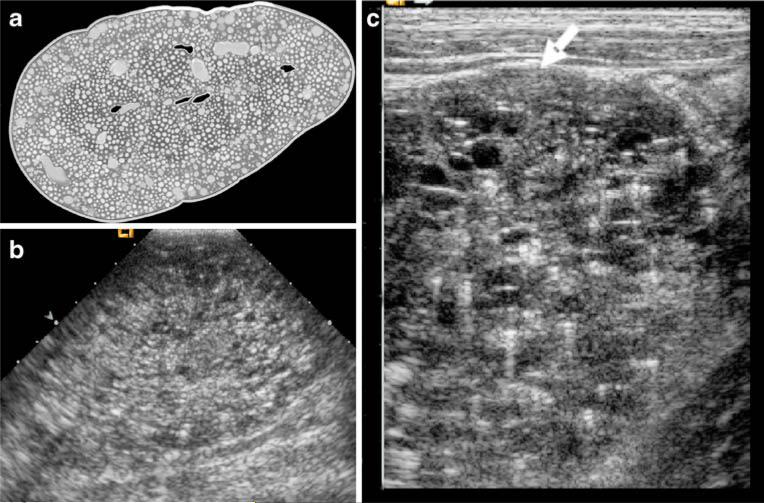
An 8-year-old girl with ARPKD/CHF. a Drawing represents complete medullary involvement with >50% cortical involvement in ARPKD. b Sagittal US image obtained with a conventional 4-MHz probe shows a diffuse severely echogenic right kidney with complete corticomedullary distinction loss. c High-resolution US image obtained with a 6-MHz probe demonstrates numerous microcysts with tiny echogenic foci invading the medulla and cortex nearly totally (>50%) with a thin preserved cortex (arrow)
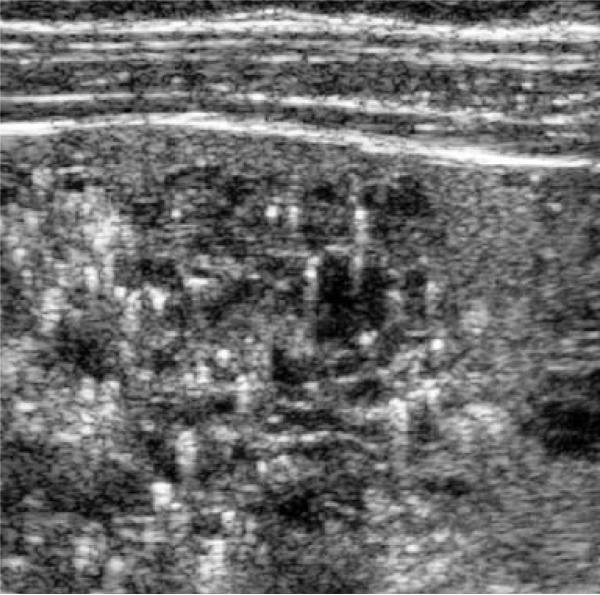
An 8-year-old boy with ARPKD/CHF. US image with a 7-MHz probe shows clusters of medullary echogenic foci without acoustic shadowing
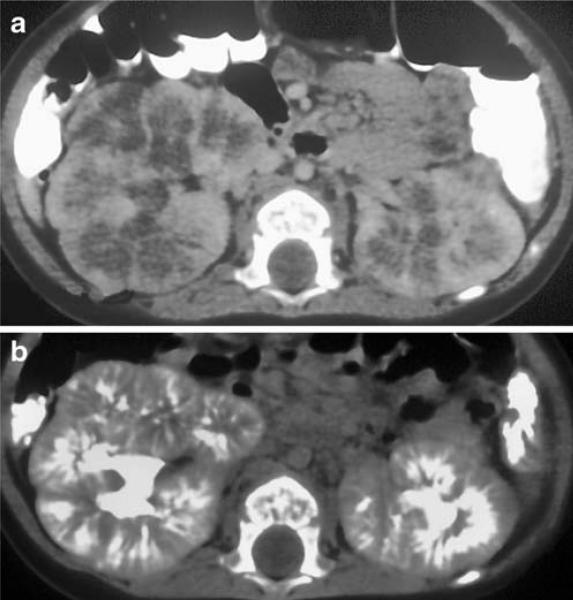
A 7-year-old girl with ARPKD/CHF. a Axial contrast-enhanced CT image in nephrographic phase demonstrates peripheral enhancement of the kidneys. b The 7-min delayed-phase image shows striated appearance of the kidneys as the excreted contrast material fills the dilated collecting ducts
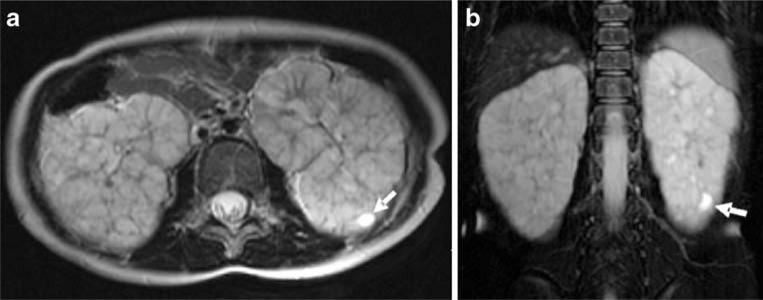
A 9-year-old girl with ARPKD/CHF. Axial (a) and coronal (b) T2-W MR images show bilateral diffusely enlarged kidneys with high signal intensity secondary to numerous corticomedullary microcysts. A macrocyst is seen at the lower pole of the left kidney (arrows)
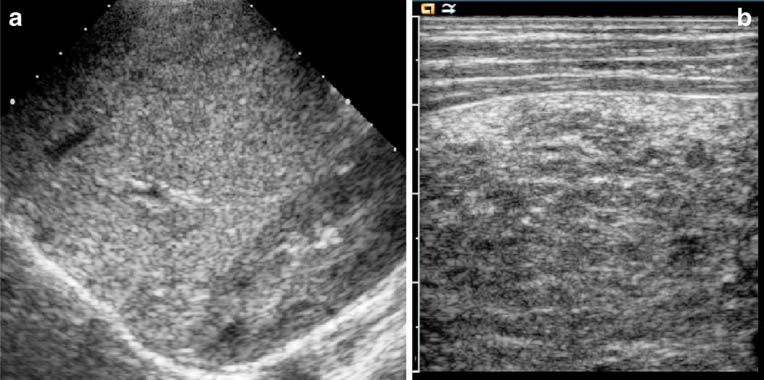
A 10-year-old boy with CHF. a Sagittal US image obtained with a conventional 4-MHz probe shows a severely echogenic liver compared with the right kidney secondary to fibrosis. b High-resolution US image obtained with a 6-MHz probe demonstrates significantly coarsened liver parenchymal echotexture
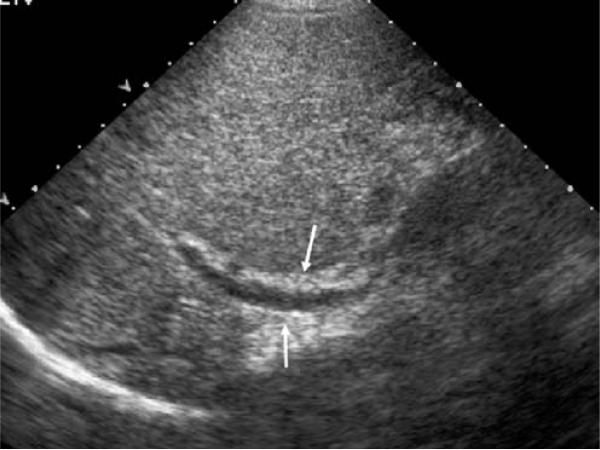
A 16-year-old-boy with CHF. US image obtained with a conventional 4-MHz probe shows moderately echogenic liver parenchyma and thickened periportal space (arrows) consistent with fibrosis
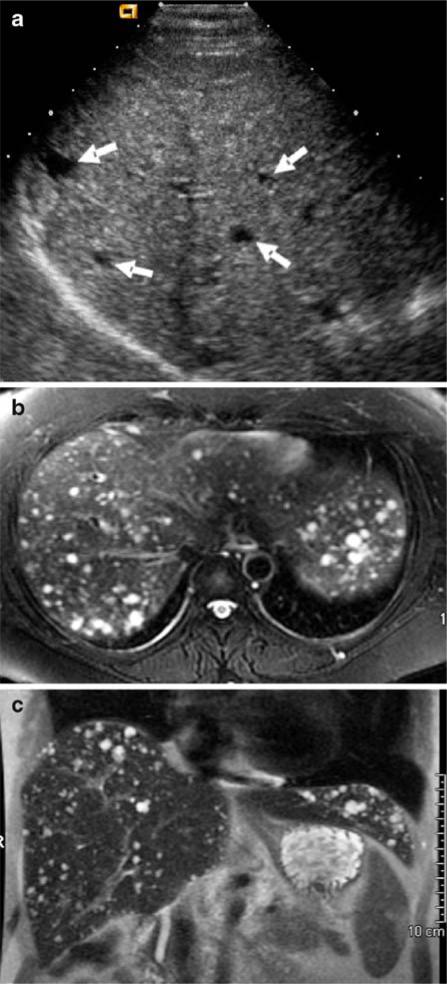
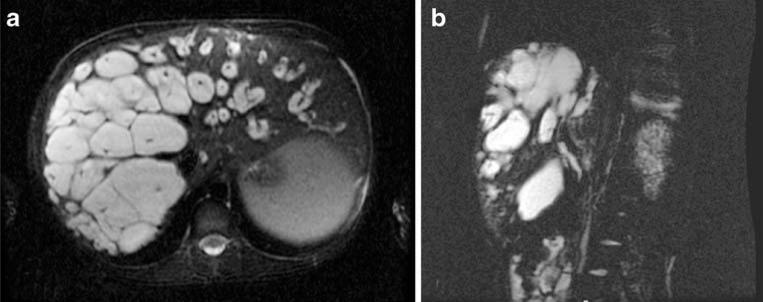
A 39-year-old woman with CHF. a US image obtained with a conventional 4-MHz probe shows numerous hypoechogenic lesions consistent with hepatic cysts (arrows). b, c T2-W MR images (b axial, c coronal) show an enlarged liver containing numerous cystic lesions along the course of the intrahepatic biliary ducts
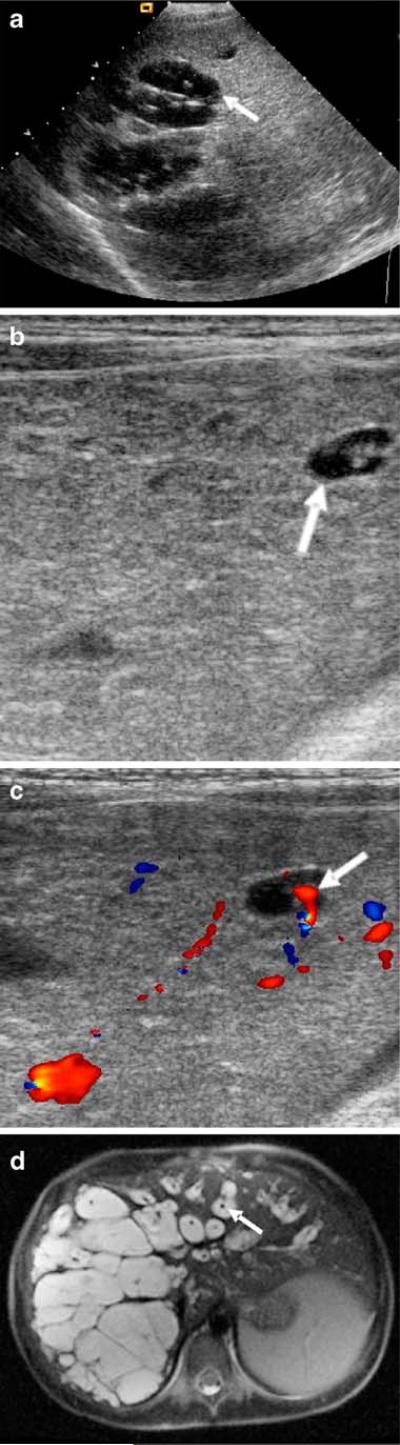
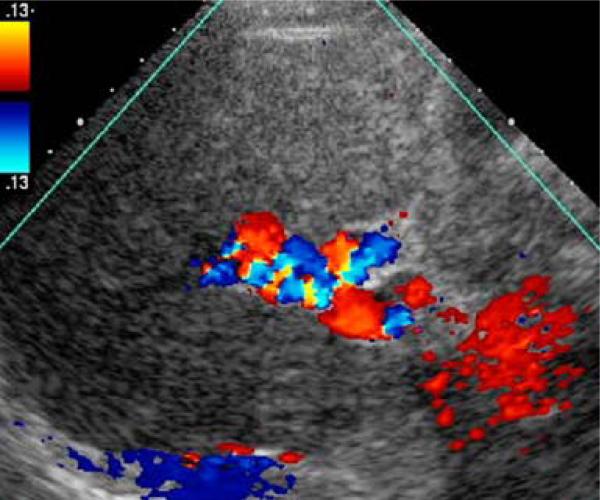
A 7-year-old boy with CHF and Caroli disease (Caroli syndrome). a US image obtained with a conventional 4-MHz probe shows clusters of macrocysts within the liver consistent with dilated intrahepatic bile ducts (arrow) and increased liver parenchymal echogenicity. b High-resolution US image obtained with a 6-MHz probe demonstrates a dilated intrahepatic bile duct with a central dot (arrow) and coarsened liver parenchyma consistent with fibrosis. c Color Doppler US image shows the flow within the central dot representing portal venous flow (arrow). d Axial T2-W MR image shows numerous biliary cysts within the liver parenchyma, some of which demonstrate the central portal vein (arrow)
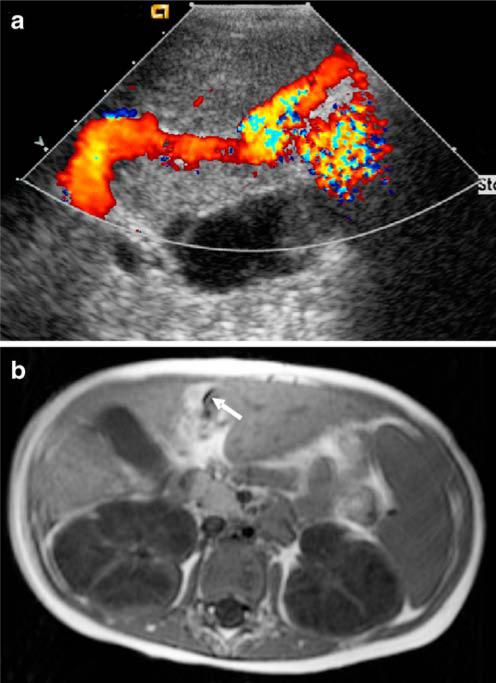
A 5½-year-old boy with CHF. a Color Doppler US image shows flow in the patent umbilical vein secondary to PH. b Axial T1-W unenhanced MR image demonstrates the patent umbilical vein (arrow)
A 35-year-old man with ARPKD/CHF. Color Doppler US image shows multiple vessels at the porta hepatis with a patent portal vein resembling the cavernomatous transformed vessels occurring secondary to portal vein obstruction
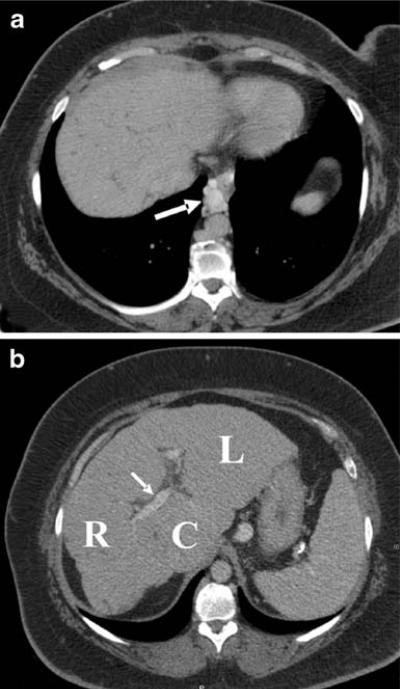
A 50-year-old woman with CHF. Axial contrast-enhanced CT images show (a) paraesophageal varicose veins (arrow) and (b) liver contour irregularity, atrophy of the right lobe (R), hypertrophy of the left (L) and caudate (C) lobes, mild periportal thickening (arrow), and splenomegaly, all of which are secondary to PH
A 7-year-old boy with Caroli syndrome (same patient as in Fig. 15). Axial (a) and reconstructed oblique (b) MR cholangiography images demonstrate dilated intrahepatic biliary ducts with the central dot sign
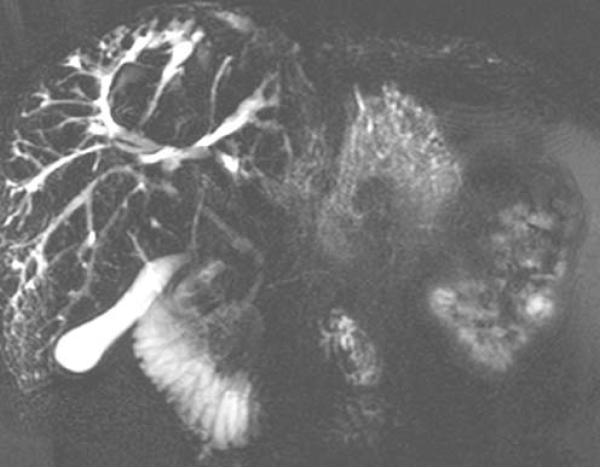
A 25-year-old man with ARPKD/CHF. Coronal MR cholangiography image demonstrates dilated peripheral intrahepatic biliary ducts and adjacent small cysts
References
-
- Zerres K, Mücher G, Becker J, et al. Prenatal diagnosis of autosomal recessive polycystic kidney disease (ARPKD): molecular genetics, clinical experience, and fetal morphology. Am J Med Genet. 1998;76:137–144. - PubMed
-
- Avner ED, Sweeney WE., Jr Renal cystic disease: new insights for the clinician. Pediatr Clin North Am. 2006;53:889–909. - PubMed
-
- Ward CJ, Hogan MC, Rossetti S, et al. The gene mutated in autosomal recessive polycystic kidney disease encodes a large, receptor-like protein. Nat Genet. 2002;30:259–269. - PubMed
-
- Bergmann C, Senderek J, Sedlacek B, et al. Spectrum of mutations in the gene for autosomal recessive polycystic kidney disease (ARPKD/PKHD1). J Am Soc Nephrol. 2003;14:76–89. - PubMed
-
- Sumfest JM, Burns MW, Mitchell ME. Aggressive surgical and medical management of autosomal recessive polycystic kidney disease. Urology. 1993;42:309–312. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
