

Effects of stent design and atherosclerotic plaque composition on arterial wall biomechanics
- PMID: 19090628
- PMCID: PMC2793418
- DOI: 10.1583/08-2443.1
Effects of stent design and atherosclerotic plaque composition on arterial wall biomechanics
Abstract
Purpose: To examine the solid mechanical effects of varying stent design and atherosclerotic plaque stiffness on the biomechanical environment induced in a diseased artery wall model.
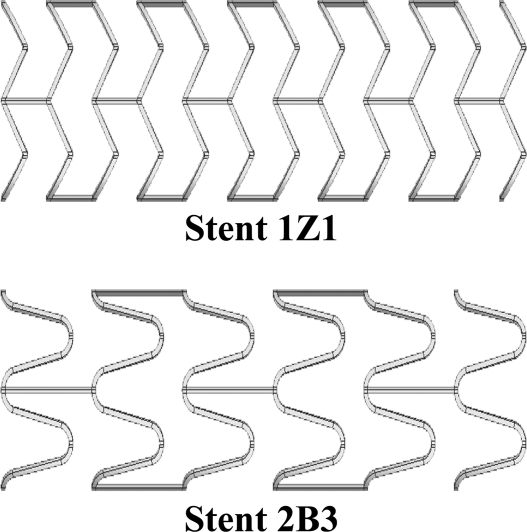
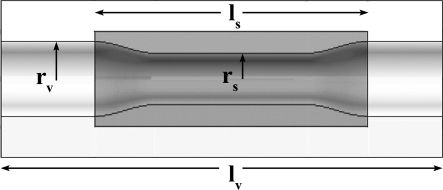
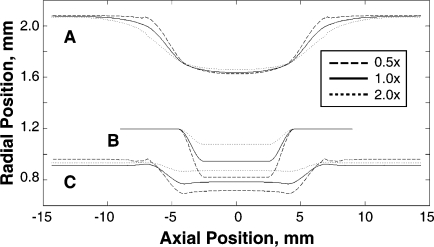
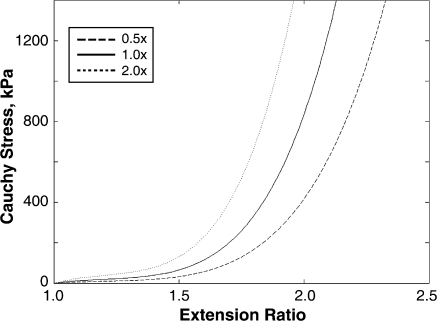
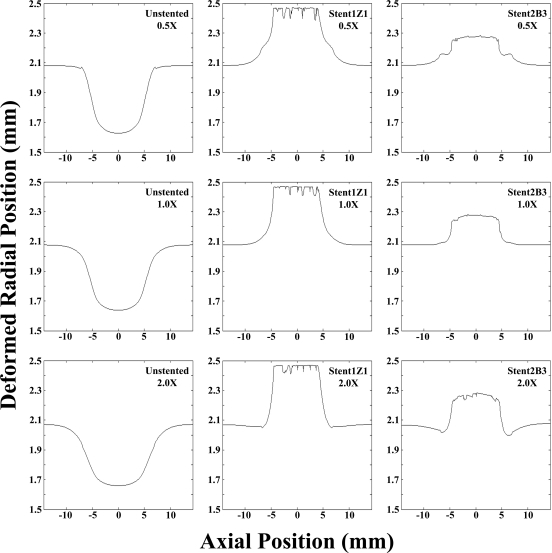
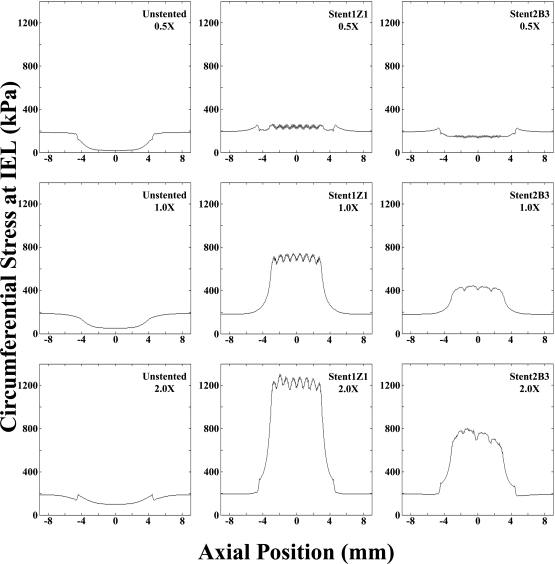
Methods: Computational modeling techniques were employed to investigate the final radius of the lumen and artery wall stresses after stent implantation. Two stent designs were studied (one stiff and one less stiff). The stenotic artery was modeled as an axisymmetrical diseased vessel with a 20% stenosis by diameter. The material properties of the diseased tissue in the artery models varied. Atherosclerotic plaques half as stiff (0.5x), of equal stiffness (1.0x), or twice as stiff (2.0x) as the artery wall were investigated.
Results: Final lumen radius was dependent on stent design, and the stiffer stent deformed the artery to an approximately 10% greater radius than the more compliant design. Alternatively, circumferential stress levels were dependent on both stent design and plaque material properties. Overall, the stiffer stent subjected the artery wall to much higher stress values than the more compliant design, with differences in peak values of 0.50, 0.31, and 0.09 MPa for the 2.0x, 1.0x, and 0.5x stiff plaques, respectively.
Conclusion: Evidence suggests that a judicious choice of stent design can minimize stress while maintaining a patent lumen in stenotic arteries. If confronted with a rigid, calcified plaque, stent design is more important, as design differences can impose dramatically different stress fields, while still providing arterial patency. Alternatively, stent design is not as much of an issue when treating a soft, lipid-laden plaque, as stress fields do not vary significantly among stent designs.
Figures
References
-
- Edelman E.R., Rogers C. Pathobiologic responses to stenting. Am J Cardiol. 1998;81:4E–6E. - PubMed
-
- Kastrati A., Mehilli J., Dirschinger J. et al. Restenosis after coronary placement of various stent types. Am J Cardiol. 2001;87:34–39. - PubMed
-
- Serruys P.W., Kutryk M.J., Ong A.T. Coronary-artery stents. N Engl J Med. 2006;354:483–495. - PubMed
-
- Joner M., Finn A.V., Farb A. et al. Pathology of drug-eluting stents in humans: delayed healing and late thrombotic risk. J Am Coll Cardiol. 2006;48:193–202. - PubMed
-
- Duda S.H., Bosiers M., Lammer J. et al. Drug-eluting and bare nitinol stents for the treatment of atherosclerotic lesions in the superficial femoral artery: long-term results from the SIROCCO trial. J Endovasc Ther. 2006;13:701–710. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
