

Sex differences in the hypertensive population with chronic ischemic heart disease
- PMID: 19090879
- PMCID: PMC8673085
- DOI: 10.1111/j.1751-7176.2008.00020.x
Sex differences in the hypertensive population with chronic ischemic heart disease
Abstract
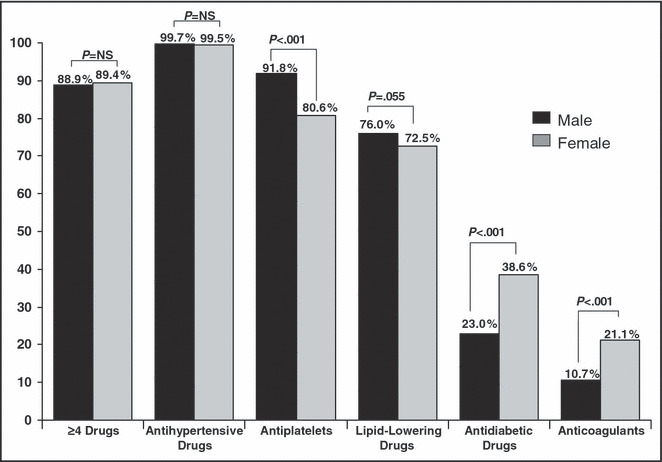
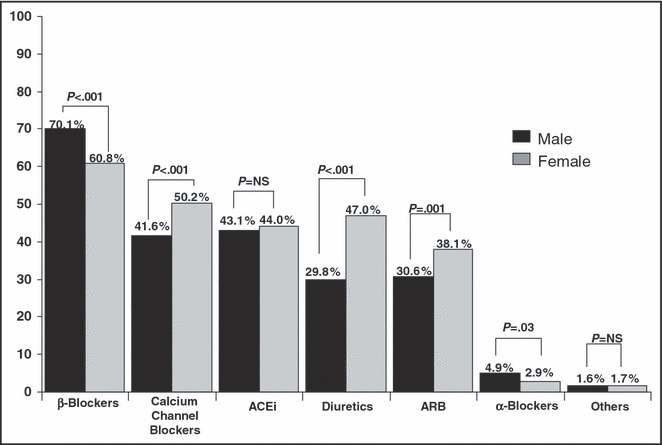
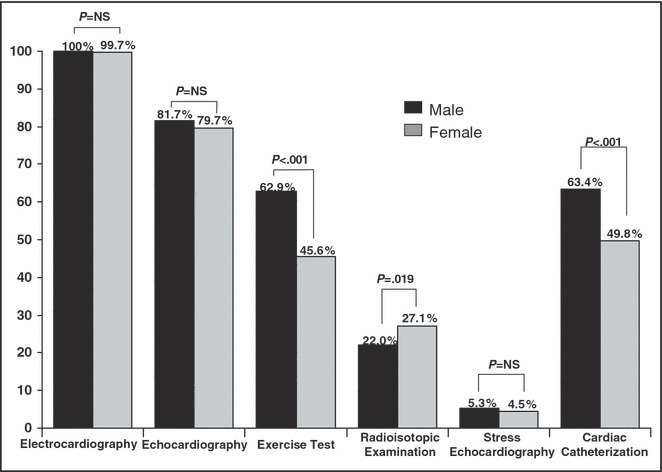
Cardiopatía Isquémica Crónica e Hipertensión Arterial en la Práctica Clínica en España (CINHTIA) was a survey designed to assess the clinical management of hypertensive outpatients with chronic ischemic heart disease. Sex differences were examined. Blood pressures (BP) was considered controlled at levels of <140/90 or <130/80 mm Hg in diabetics (European Society of Hypertension/European Society of Cardiology 2003); low-density lipoprotein cholesterol (LDL-C) was considered controlled at levels <100 mg/dL (National Cholesterol Education Program Adult Treatment Panel III). In total, 2024 patients were included in the study. Women were older, with a higher body mass index and an increased prevalence of atrial fibrillation. Dyslipidemia, smoking, sedentary lifestyle, and peripheral arterial disease were more frequent in men. In contrast, diabetes, left ventricular hypertrophy, and heart failure were more common in women. BP and LDL-C control rates, although poor in both groups, were better in men (44.9% vs 30.5%, P<.001 and 33.0% vs 25.0%, P<.001, respectively). Stress testing and coronary angiography were more frequently performed in men.
Figures

References
-
- Fox CS, Evans JC, Larson MG, et al. Temporal trends in coronary heart disease mortality and sudden cardiac death from 1950 to 1999. The Framingham Heart Study. Circulation. 2004;110:522–527. - PubMed
-
- Mosca L, Banka CL, Benjamin EJ, et al. Evidence‐based guidelines for cardiovascular disease prevention in women: 2007 update. Circulation. 2007;115:1481–1501. - PubMed
-
- Mosca L, Linfante AH, Benjamin EJ, et al. National study of physician awareness and adherence to cardiovascular disease prevention guidelines in the United States. Circulation. 2005;111:499–510. - PubMed
-
- Mosca L, Appel LJ, Benjamin EJ, et al. Evidence‐based guidelines for cardiovascular disease prevention in women. J Am Coll Cardiol. 2004;43:900–921. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
