

Incidence, organ dysfunction and mortality in severe sepsis: a Spanish multicentre study
- PMID: 19091069
- PMCID: PMC2646323
- DOI: 10.1186/cc7157
Incidence, organ dysfunction and mortality in severe sepsis: a Spanish multicentre study
Abstract
Introduction: Sepsis is a leading cause of admission to non-cardiological intensive care units (ICUs) and the second leading cause of death among ICU patients. We present the first extensive dataset on the epidemiology of severe sepsis treated in ICUs in Spain.
Methods: We conducted a prospective, observational, multicentre cohort study, carried out over two 3-month periods in 2002. Our aims were to determine the incidence of severe sepsis among adults in ICUs in a specific area in Spain, to determine the early (48 h) ICU and hospital mortality rates, as well as factors associated with the risk of death.
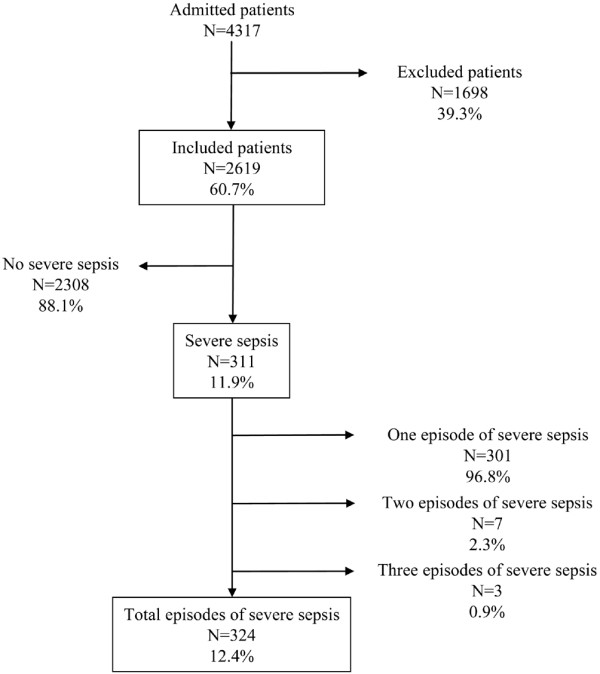
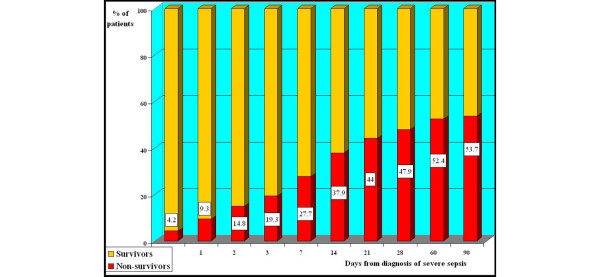
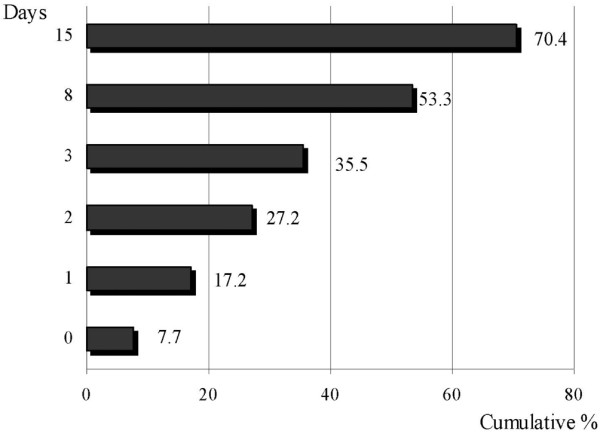
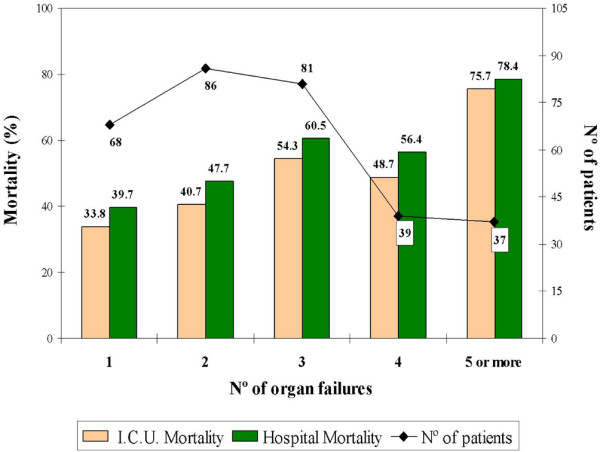
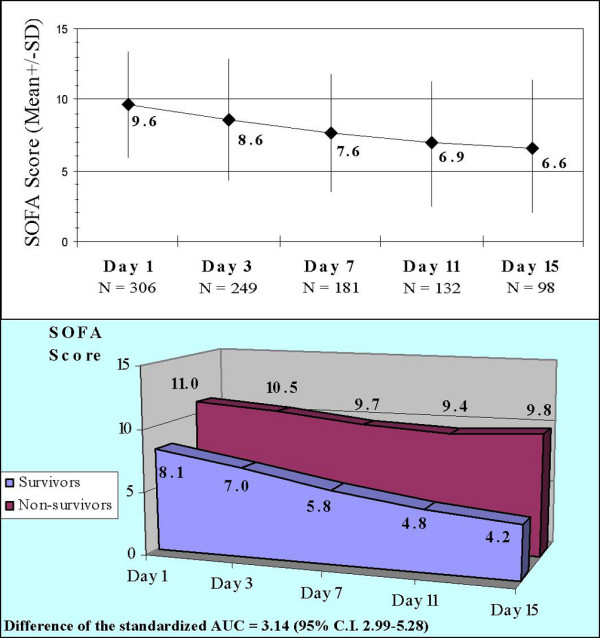
Results: A total of 4,317 patients were admitted and 2,619 patients were eligible for the study; 311 (11.9%) of these presented at least 1 episode of severe sepsis, and 324 (12.4%) episodes of severe sepsis were recorded. The estimated accumulated incidence for the population was 25 cases of severe sepsis attended in ICUs per 100,000 inhabitants per year. The mean logistic organ dysfunction system (LODS) upon admission was 6.3; the mean sepsis-related organ failure assessment (SOFA) score on the first day was 9.6. Two or more organ failures were present at diagnosis in 78.1% of the patients. A microbiological diagnosis of the infection was reached in 209 episodes of sepsis (64.5%) and the most common clinical diagnosis was pneumonia (42.8%). A total of 169 patients (54.3%) died in hospital, 150 (48.2%) of these in the ICU. The mortality in the first 48 h was 14.8%. Factors associated with early death were haematological failure and liver failure at diagnosis, acquisition of the infection prior to ICU admission, and total LODS score on admission. Factors associated with death in the hospital were age, chronic alcohol abuse, increased McCabe score, higher LODS on admission, DeltaSOFA 3-1 (defined as the difference in the total SOFA scores on day 3 and on day 1), and the difference of the area under the curve of the SOFA score throughout the first 15 days.
Conclusions: We found a high incidence of severe sepsis attended in the ICU and high ICU and hospital mortality rates. The high prevalence of multiple organ failure at diagnosis and the high mortality in the first 48 h suggests delays in diagnosis, in initial resuscitation, and/or in initiating appropriate antibiotic treatment.
Figures
Comment in
-
Extending international sepsis epidemiology: the impact of organ dysfunction.Crit Care. 2009;13(1):120. doi: 10.1186/cc7704. Epub 2009 Feb 23. Crit Care. 2009. PMID: 19291262 Free PMC article. Review.
References
-
- Bone RC, Balk RA, Cerra FB, Dellinger RP, Fein AM, Knaus WA, Schein RM, Sibbald WJ. Definition for sepsis and organ failure and guidelines for use of innovative therapies in sepsis. The ACCP/SCCM Consensus Conference Committee. American College of Chest Physicians/Society of Critical Care Medicine. Chest. 1992;101:1644–1655. doi: 10.1378/chest.101.6.1644. - DOI - PubMed
-
- Brun-Buisson C, Doyon F, Carlet J, Dellamonica P, Gouin F, Lepoutre A, Mercier JC, Offenstadt G, Régnier B. Incidence, risk factors, and outcome of severe sepsis and septic shock in adults. A multicenter prospective study in intensive care units. French ICU Group for Severe Sepsis. JAMA. 1995;274:968–974. doi: 10.1001/jama.274.12.968. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
