

Astigmatism in the Early Treatment for Retinopathy Of Prematurity Study: findings to 3 years of age
- PMID: 19091409
- PMCID: PMC2692212
- DOI: 10.1016/j.ophtha.2008.09.035
Astigmatism in the Early Treatment for Retinopathy Of Prematurity Study: findings to 3 years of age
Abstract
Purpose: To examine the prevalence of astigmatism (> or =1.00 diopter [D]) and high astigmatism (> or =2.00 D) at 6 and 9 months corrected age and 2 and 3 years postnatal age, in preterm children with birth weight of less than 1251 g in whom high-risk prethreshold retinopathy of prematurity (ROP) developed and who participated in the Early Treatment for Retinopathy of Prematurity (ETROP) Study.
Design: Randomized, controlled clinical trial.
Participants: Four hundred one infants in whom prethreshold ROP developed in one or both eyes and who were randomized after they were determined to have a high risk (> or =15%) of poor structural outcome without treatment using the Risk Management of Retinopathy of Prematurity (RM-ROP2) program. Refractive error was measured by cycloplegic retinoscopy. Eyes with additional retinal, glaucoma, or cataract surgery were excluded.
Intervention: Eyes were randomized to receive laser photocoagulation at high-risk prethreshold ROP (early treated [ET]) or to be conventionally managed (CM), receiving treatment only if threshold ROP developed.
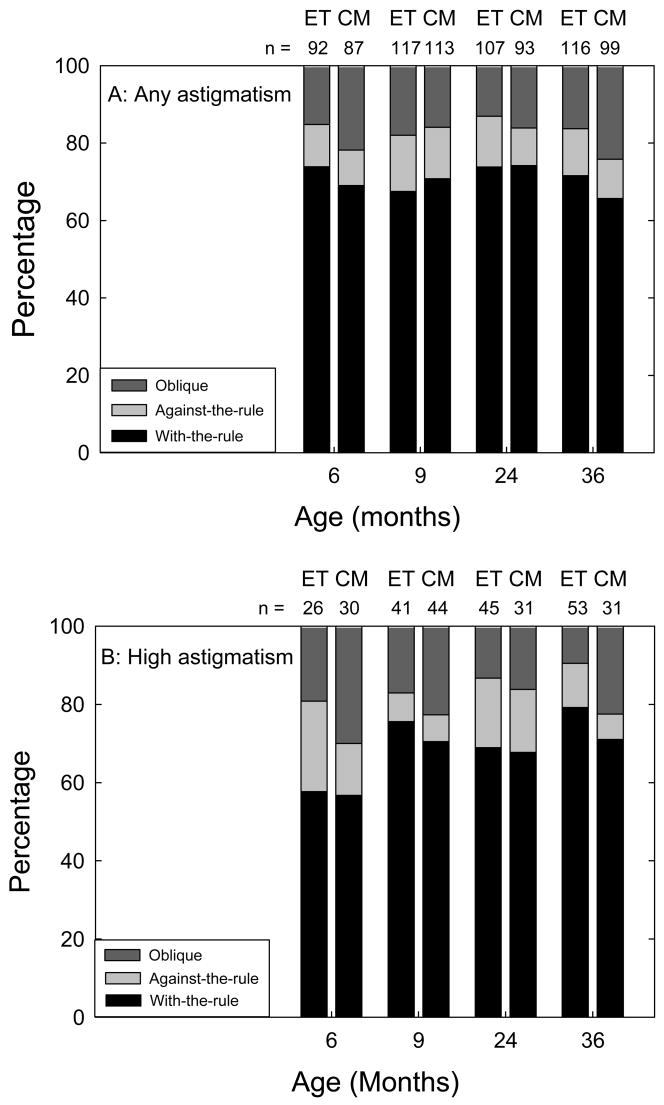
Main outcome measures: Astigmatism and high astigmatism at each visit. Astigmatism was classified as with-the-rule (WTR; 75 degrees -105 degrees ), against-the-rule (ATR; 0 degrees -15 degrees and 165 degrees -180 degrees ), or oblique (OBL; 16 degrees -74 degrees and 106 degrees -164 degrees ).
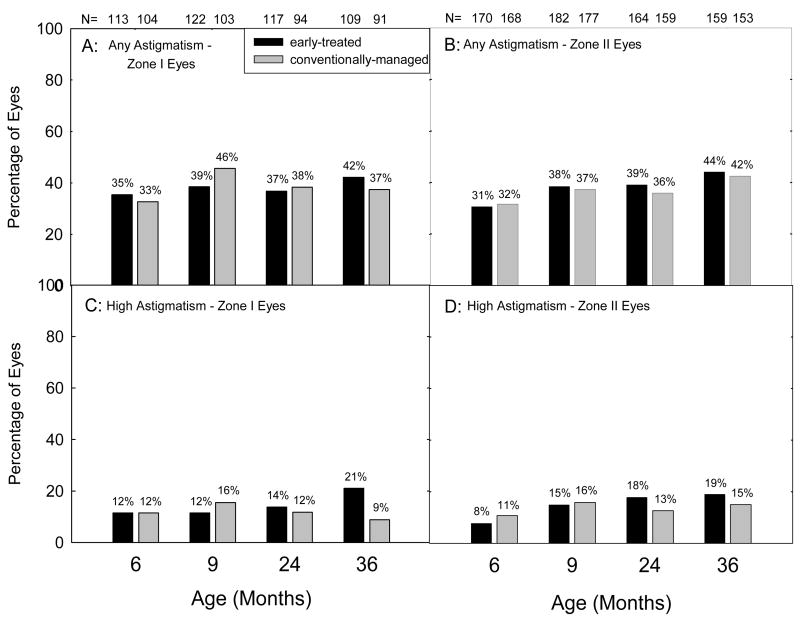
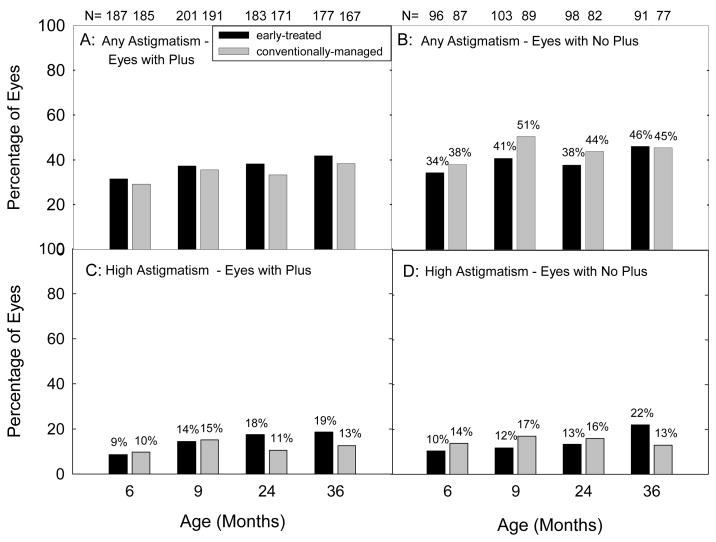
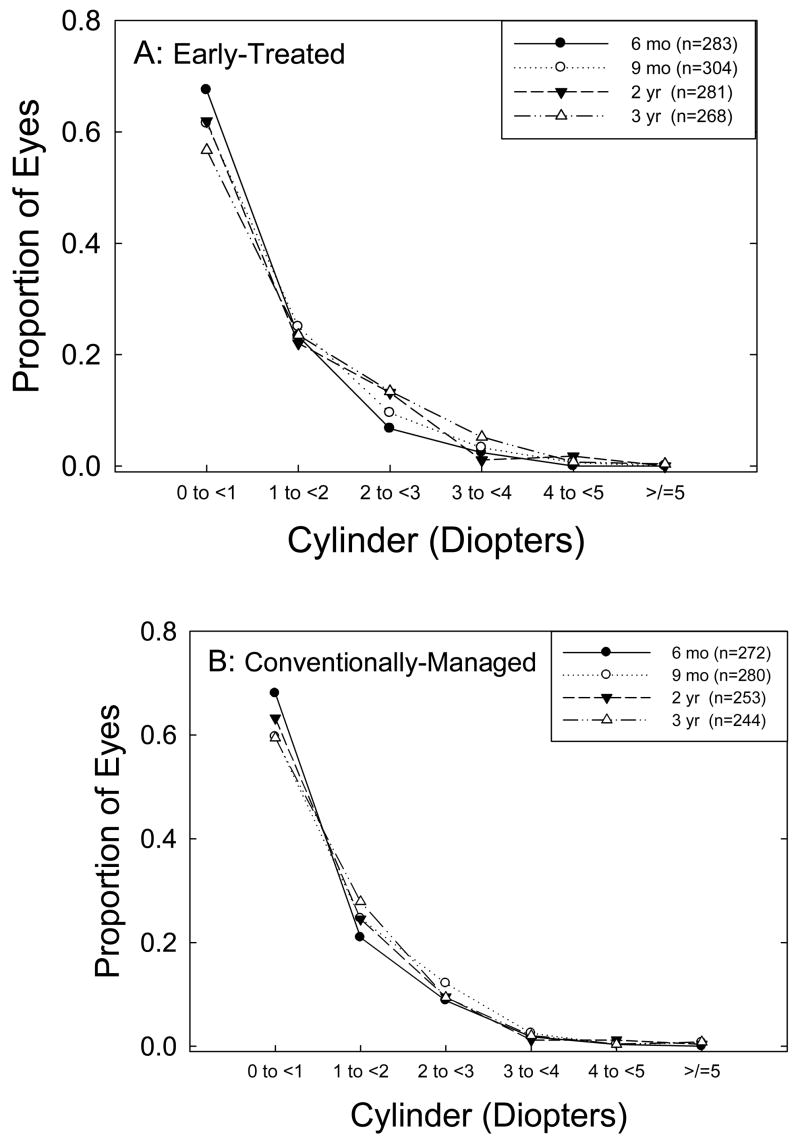
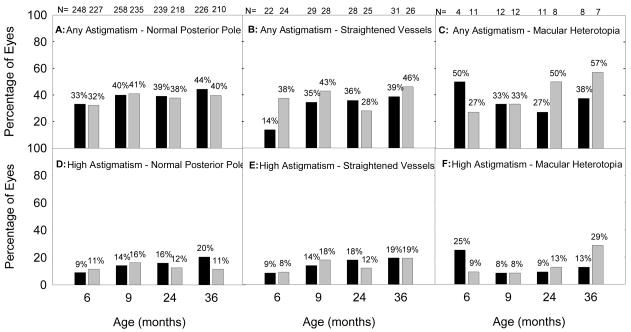
Results: The prevalence of astigmatism in ET and CM eyes was similar at each test age. For both groups, there was an increase in prevalence of astigmatism from approximately 32% at 6 months to approximately 42% by 3 years, mostly occurring between 6 and 9 months. Among eyes that could be refracted, astigmatism was not influenced by zone of acute-phase ROP, presence of plus disease, or retinal residua of ROP. Eyes with astigmatism and high astigmatism most often had WTR astigmatism.
Conclusions: By age 3 years, nearly 43% of eyes treated at high-risk prethreshold ROP developed astigmatism of > or =1.00 D and nearly 20% had astigmatism of > or =2.00 D. Presence of astigmatism was not influenced by timing of treatment of acute-phase ROP or by characteristics of acute-phase or cicatricial ROP. These findings reinforce the need for follow-up eye examinations in infants with high-risk prethreshold ROP.
Financial disclosure(s): The author(s) have no proprietary or commercial interest in any materials discussed in this article.
Figures
References
-
- Dobson V, Fulton AB, Manning K, et al. Cycloplegic refractions of premature infants. Am J Ophthalmol. 1981;91:490–5. - PubMed
-
- Varughese S, Varghese RM, Gupta N, et al. Refractive error at birth and its relation to gestational age. Curr Eye Res. 2005;30:423–8. - PubMed
-
- Larsson EK, Holmström GE. Development of astigmatism and anisometropia in preterm children during the first 10 years of life: a population-based study. Arch Ophthalmol. 2006;124:1608–14. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
