

Treatment effects for which shift or binary analyses are advantageous in acute stroke trials
- PMID: 19092107
- PMCID: PMC2677490
- DOI: 10.1212/01.wnl.0000341308.73506.b7
Treatment effects for which shift or binary analyses are advantageous in acute stroke trials
Abstract
Background: In acute stroke trials, functional outcome may be analyzed by dichotomizing ordinal outcome scales or by evaluating the entire scale range (shift analysis). The conditions under which shift or binary analysis will be more efficient have not been previously well delineated.
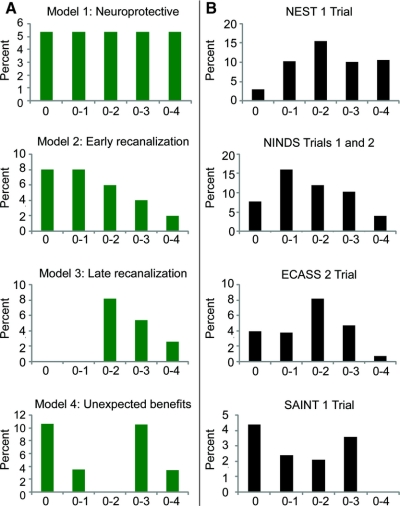
Methods: Model randomized clinical trials employing the modified Rankin Scale of global handicap were constructed to reflect 1) mild benefits experienced across all ranges of stroke severity (neuroprotective effect), 2) substantial benefits across all ranges of stroke severity (early recanalization effect), 3) substantial benefits across wide range of stroke severity but with limited ability to achieve fully normal outcome (late recanalization effect), 4) benefits clustered at unexpected health state transitions.
Results: In neuroprotective models, shift analysis was the most efficient technique in detecting a treatment effect. In the early recanalization models, dichotomization at excellent outcome and shift analysis were of comparable efficiency, both superior to dichotomization at good outcome. In the late recanalization models, dichotomization at good outcome performed best, shift analysis less well, and dichotomization at excellent outcome poorly. In the unexpected benefits model, shift analysis substantially outperformed dichotomization analyses. These patterns held among the seven actual acute trials reporting full range Rankin outcomes and showing treatment benefit identified in the literature.
Conclusions: The pattern of treatment effect of the intervention determines whether shift analysis or simple dichotomized analysis will be more efficient. Shift analysis is especially advantageous when treatments confer a relatively uniform, mild benefit to patients over a wide range of stroke severities or confer benefits at unexpected but clinically important health state transitions.
Figures

Comment in
-
Stroke trials: a shift to shift analysis?Neurology. 2009 Apr 14;72(15):1292-3. doi: 10.1212/WNL.0b013e3181a11417. Neurology. 2009. PMID: 19365050 No abstract available.
References
-
- Lees KR, Zivin JA, Ashwood T, et al. NXY-059 for acute ischemic stroke. N Engl J Med 2006;354:588–600. - PubMed
-
- Saver JL. Novel end point analytic techniques and interpreting shifts across the entire range of outcome scales in acute stroke trials. Stroke 2007;38:3055–3062. - PubMed
-
- Bath PM, Gray LJ, Collier T, Pocock S, Carpenter J. Can we improve the statistical analysis of stroke trials? Statistical reanalysis of functional outcomes in stroke trials. Stroke 2007;38:1911–1915. - PubMed
-
- The National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group. Tissue plasminogen activator for acute ischemic stroke. N Engl J Med 1995;333:1581–1587. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical