

Recovery of activities of daily living in older adults after hospitalization for acute medical illness
- PMID: 19093915
- PMCID: PMC2717728
- DOI: 10.1111/j.1532-5415.2008.02023.x
Recovery of activities of daily living in older adults after hospitalization for acute medical illness
Abstract
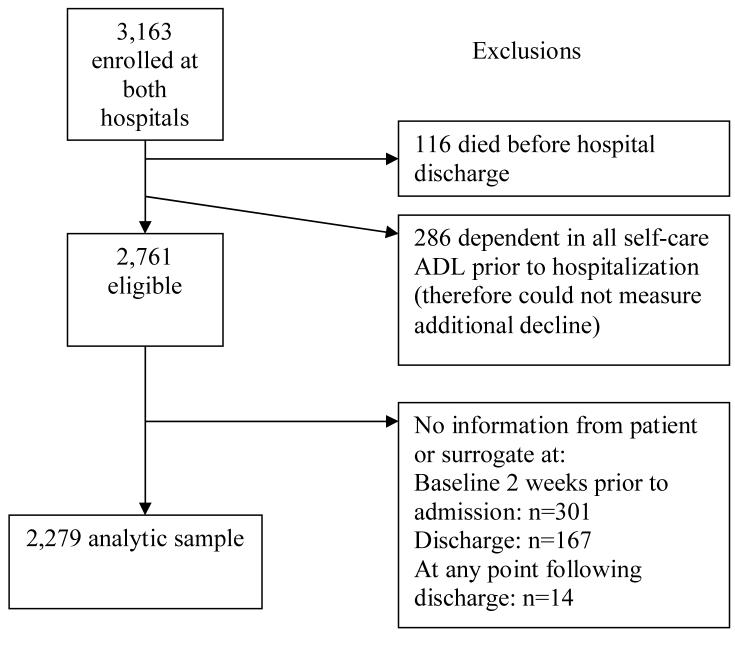
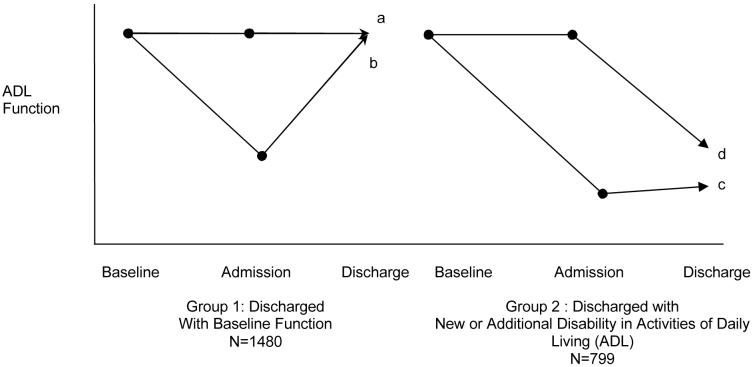
Objectives: To compare functional outcomes in the year after discharge for older adults discharged from the hospital after an acute medical illness with a new or additional disability in their basic self-care activities of daily living (ADL) (compared with preadmission baseline 2 weeks before admission) with those of older adults discharged with baseline ADL function and identify predictors of failure to recover to baseline function 1 year after discharge.
Design: Observational.
Setting: Tertiary care hospital, community teaching hospital.
Participants: Older (aged >or=70) patients nonelectively admitted to general medical services (1993-1998).
Measurements: Number of ADL disabilities at preadmission baseline and 1, 3, 6, and 12 months after discharge. Outcomes were death, sustained decline in ADL function, and recovery to baseline ADL function at each time point.
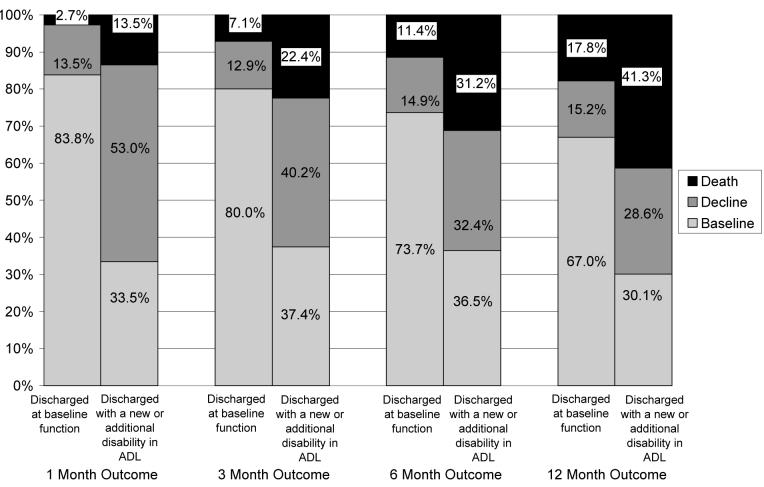
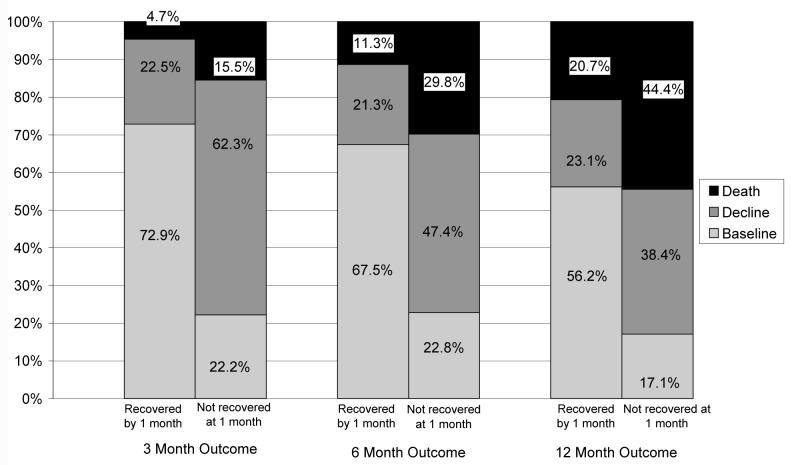
Results: By 12 months after discharge, of those discharged with new or additional ADL disability, 41.3% died, 28.6% were alive but had not recovered to baseline function, and 30.1% were at baseline function. Of those discharged at baseline function, 17.8% died, 15.2% were alive but with worse than baseline function, and 67% were at their baseline function (P<.001). Of those discharged with new or additional ADL disability, the presence or absence of recovery by 1 month was associated with long-term outcomes. Age, cardiovascular disease, dementia, cancer, low albumin, and greater number of dependencies in instrumental ADLs independently predicted failure to recover.
Conclusion: For older adults discharged with new or additional disability in ADL after hospitalization for medical illness, prognosis for functional recovery is poor. Rehabilitation interventions of longer duration and timing than current reimbursement allows, caregiver support, and palliative care should be evaluated.
Figures
Comment in
-
Motor recovery after rehabilitation and long-term clinical outcomes.J Am Geriatr Soc. 2009 Jul;57(7):1300-1. doi: 10.1111/j.1532-5415.2009.02310.x. J Am Geriatr Soc. 2009. PMID: 19570159 No abstract available.
References
-
- Ferrucci L, Guralnik JM, Simonsick E, et al. Progressive versus catastrophic disability: A longitudinal view of the disablement process. J Gerontol A Biol Sci Med Sci. 1996;51:M123–130. - PubMed
-
- Gill TM, Williams CS, Tinetti ME. The combined effects of baseline vulnerability and acute hospital events on the development of functional dependence among community-living older persons. J Gerontol A Biol Sci Med Sci. 1999;54:M377–383. - PubMed
-
- Ferrucci L, Guralnik JM, Pahor M, et al. Hospital diagnoses, Medicare charges, and nursing home admissions in the year when older persons become severely disabled. JAMA. 1997;277:728–734. - PubMed
-
- Sager MA, Rudberg MA, Jalaluddin M, et al. Hospital admission risk profile (HARP): identifying older patients at risk for functional decline following acute medical illness and hospitalization. J Am Geriatr Soc. 1996;44:251–257. - PubMed
-
- Boyd CM, Xue QL, Guralnik JM, et al. Hospitalization and development of dependence in dctivities of daily living in a cohort of disabled older women: The Women’s Health and Aging Study I. J Gerontol A Biol Sci Med Sci. 2005;60:888–893. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
