

Tolerability, pharmacokinetics and night-time effects on postural sway and critical flicker fusion of gaboxadol and zolpidem in elderly subjects
- PMID: 19094161
- PMCID: PMC2670375
- DOI: 10.1111/j.1365-2125.2008.03331.x
Tolerability, pharmacokinetics and night-time effects on postural sway and critical flicker fusion of gaboxadol and zolpidem in elderly subjects
Abstract
What is already known about this subject: Body sway increases in older adults and may lead to an increase in the risk of falling. The problem of impaired stability in the elderly may be compounded by the use of hypnotics, which have been associated with an increased risk of next-day falls as well as drowsiness. The potential adverse effects of hypnotic drugs on steadiness may be exacerbated during the night, in the event that an individual needs to get out of bed.
What this study adds: This study examines the effects of gaboxadol (an investigational treatment for insomnia), zolpidem (a current hypnotic included as an active control) and placebo on body sway and attention/information processing ability following bedtime dosing in elderly subjects who were woken during the night for assessments. Zolpidem and gaboxadol increased body sway at various time points during the night relative to placebo; at 1.5 h post dose, the time of peak concentrations of both drugs, gaboxadol produced less impairment than zolpidem. Compared with placebo, neither gaboxadol nor zolpidem impaired attention/information-processing ability as assessed by critical flicker fusion.
Aims: To evaluate tolerability, pharmacokinetics and night-time effects on body sway and critical flicker fusion (CFF) of gaboxadol following bedtime dosing in healthy elderly subjects.
Methods: Subjects (17 women, seven men) aged 65-75 years received gaboxadol 10 mg, zolpidem 5 mg (active control) or placebo at 22.00 h in a three-period, randomized, double-blind crossover study. They were awakened during the night for evaluation of body sway and CFF. Pharmacokinetics of gaboxadol were assessed during a fourth single-blind treatment period. Adverse events were recorded throughout the study.
Results: The number of subjects with adverse events was 14 for gaboxadol 10 mg, seven for zolpidem and nine for placebo; most were mild or moderate in intensity. Two women discontinued the study following gaboxadol; one vomited and one experienced a severe vasovagal syncope after venepuncture. Mean gaboxadol t(max) was 2 h, t((1/2)) was 1.7 h, AUC(0-infinity) was 430 ng.h ml(-1) and C(max) was 139 ng ml(-1). At 1.5 h and 4 h post dose, zolpidem increased body sway relative to placebo (P < 0.01). Gaboxadol increased body sway at 4 h (P < 0.001) and 8 h (P < 0.05) relative to placebo. At 1.5 h, the time point closest to peak drug concentrations, zolpidem increased body sway compared with gaboxadol (P < 0.01). Gaboxadol and zolpidem had no effects on CFF vs. placebo.
Conclusions: A bedtime dose of gaboxadol 10 mg was generally well tolerated. Changes in body sway at 1.5 h after bedtime dosing were smaller with gaboxadol 10 mg than with zolpidem 5 mg, whereas changes were similar at 4 h for both treatments and returned to near baseline at 8 h.
Figures
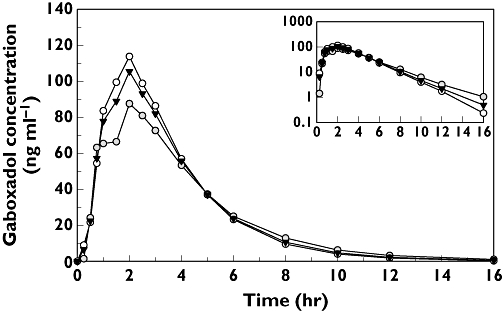
 ); Women (n = 15) (○); Overall (n = 22) (▾)
); Women (n = 15) (○); Overall (n = 22) (▾)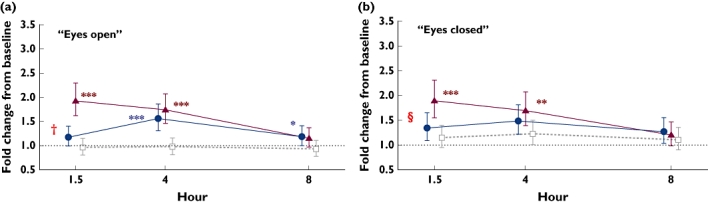
 )
)References
-
- Chiu HF, Leung T, Lam LCW, Wing YK, Chung DWS, Li SW, Chi I, Law WT, Boey KW. Sleep problems in Chinese elderly in Hong Kong. Sleep. 1999;22:717–26. - PubMed
-
- Foley DJ, Monjan AA, Brown SL, Simonsick EM, Wallace RB, Blazer DG. Sleep complaints among elderly persons – an epidemiologic study of 3 communities. Sleep. 1995;18:425–32. - PubMed
-
- Bliwise DL. Sleep in normal aging and dementia. Sleep. 1993;16:40–81. - PubMed
-
- Ohayon MM, Carskadon MA, Guilleminault C, Vitiello MV. Meta-analysis of quantitative sleep parameters from childhood to old age in healthy individuals: developing normative sleep values across the human lifespan. Sleep. 2004;27:1255–73. - PubMed
-
- Phillips B, Ancoli-Israel S. Sleep disorders in the elderly. Sleep Med. 2001;2:99–114. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
