

A systematic review and meta-analysis of the effects of clinical pathways on length of stay, hospital costs and patient outcomes
- PMID: 19094244
- PMCID: PMC2632661
- DOI: 10.1186/1472-6963-8-265
A systematic review and meta-analysis of the effects of clinical pathways on length of stay, hospital costs and patient outcomes
Abstract
Background: To perform a systematic review about the effect of using clinical pathways on length of stay (LOS), hospital costs and patient outcomes. To provide a framework for local healthcare organisations considering the effectiveness of clinical pathways as a patient management strategy.
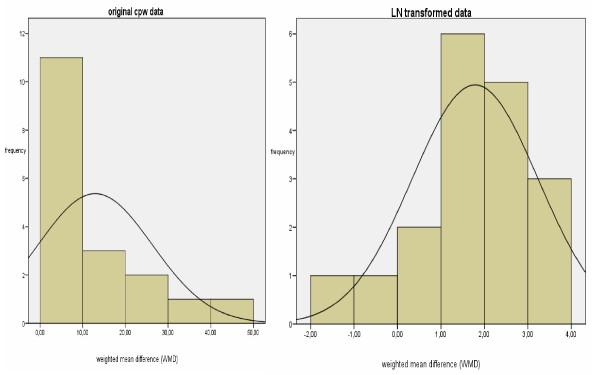
Methods: As participants, we considered hospitalized children and adults of every age and indication whose treatment involved the management strategy "clinical pathways". We include only randomised controlled trials (RCT) and controlled clinical trials (CCT), not restricted by language or country of publication. Single measures of continuous and dichotomous study outcomes were extracted from each study. Separate analyses were done in order to compare effects of clinical pathways on length of stay (LOS), hospital costs and patient outcomes. A random effects meta-analysis was performed with untransformed and log transformed outcomes.
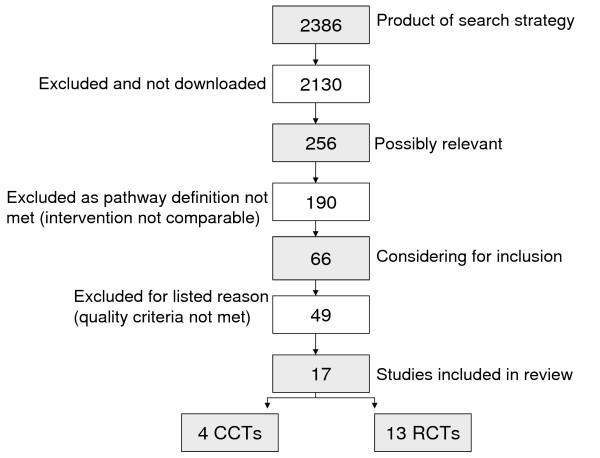
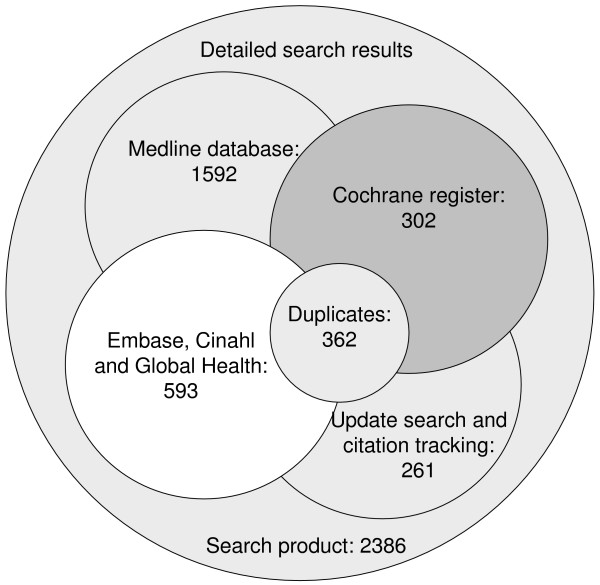
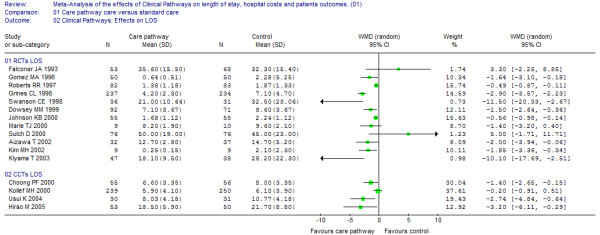
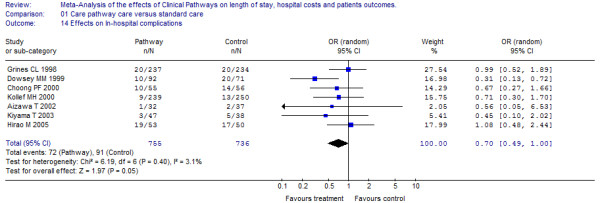
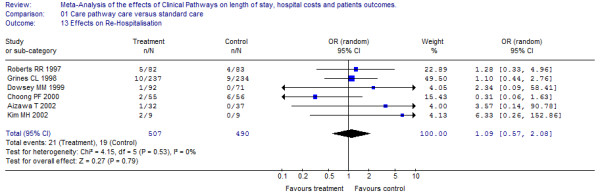
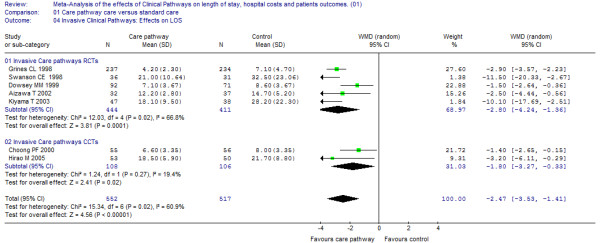
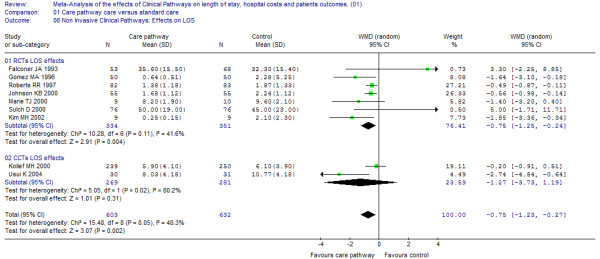
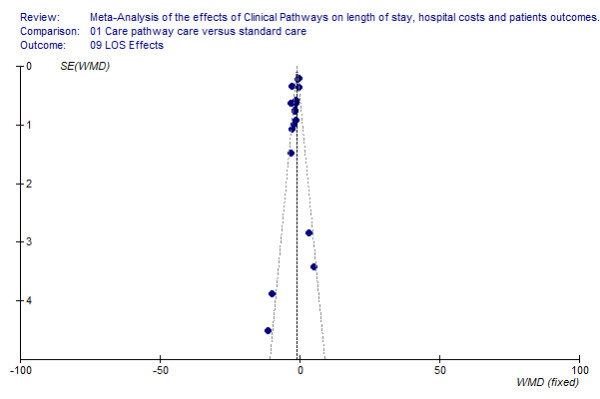
Results: In total 17 trials met inclusion criteria, representing 4,070 patients. The quality of the included studies was moderate and studies reporting economic data can be described by a very limited scope of evaluation. In general, the majority of studies reporting economic data (LOS and hospital costs) showed a positive impact. Out of 16 reporting effects on LOS, 12 found significant shortening. Furthermore, in a subgroup-analysis, clinical pathways for invasive procedures showed a stronger LOS reduction (weighted mean difference (WMD) -2.5 days versus -0.8 days)).There was no evidence of differences in readmission to hospitals or in-hospital complications. The overall Odds Ratio (OR) for re-admission was 1.1 (95% CI: 0.57 to 2.08) and for in-hospital complications, the overall OR was 0.7 (95% CI: 0.49 to 1.0). Six studies examined costs, and four showed significantly lower costs for the pathway group. However, heterogeneity between studies reporting on LOS and cost effects was substantial.
Conclusion: As a result of the relatively small number of studies meeting inclusion criteria, this evidence base is not conclusive enough to provide a replicable framework for all pathway strategies. Considering the clinical areas for implementation, clinical pathways seem to be effective especially for invasive care. When implementing clinical pathways, the decision makers need to consider the benefits and costs under different circumstances (e.g. market forces).
Figures
References
-
- Coffey RJ, Richards JS, Remmert CS, LeRoy SS, Schoville RR, Baldwin PJ. An introduction to critical paths. Qual Manag Health Care. 2005;14:46–55. - PubMed
-
- Saint S, Hofer TP, Rose JS, Kaufman SR, McMahon LF., Jr Use of critical pathways to improve efficiency: a cautionary tale. Am J Manag Care. 2003;9:758–765. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
